




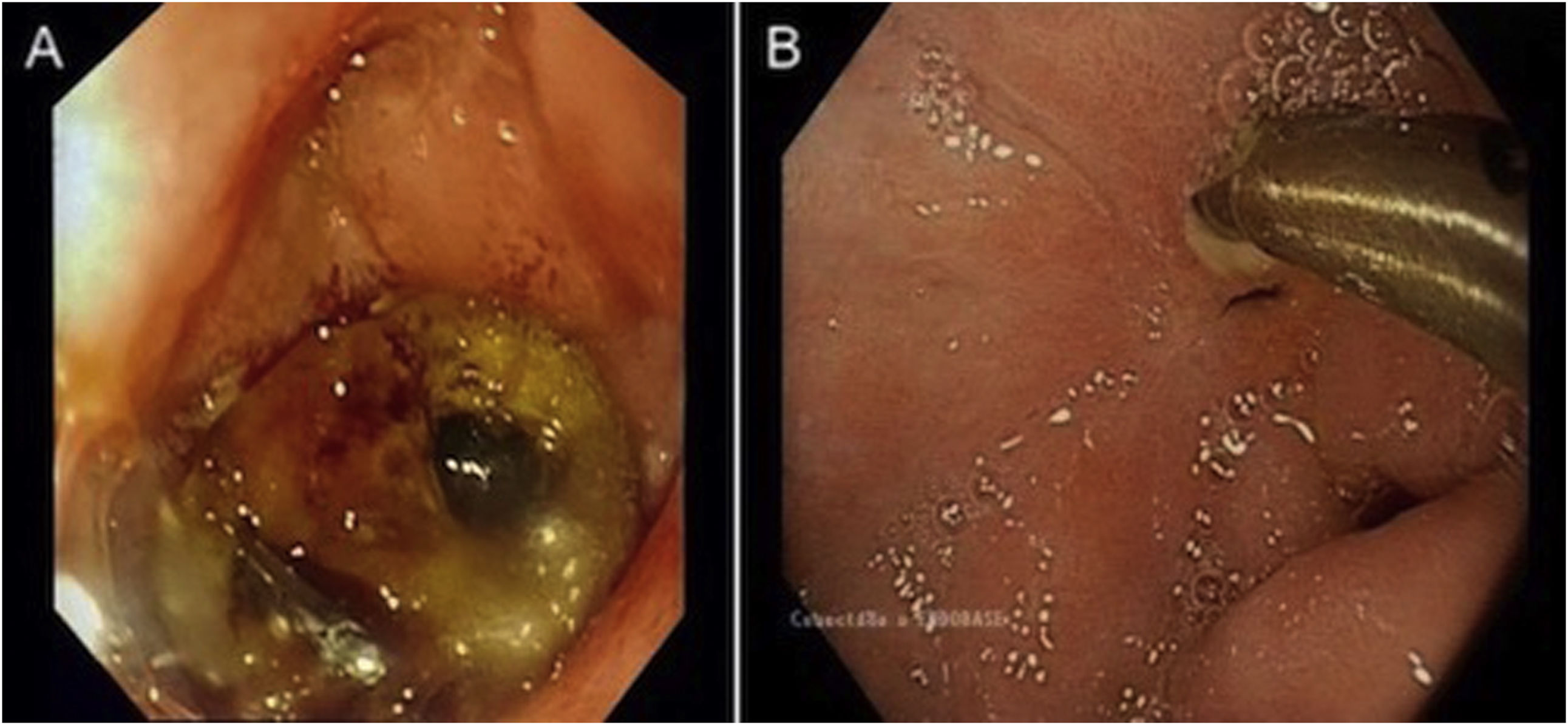
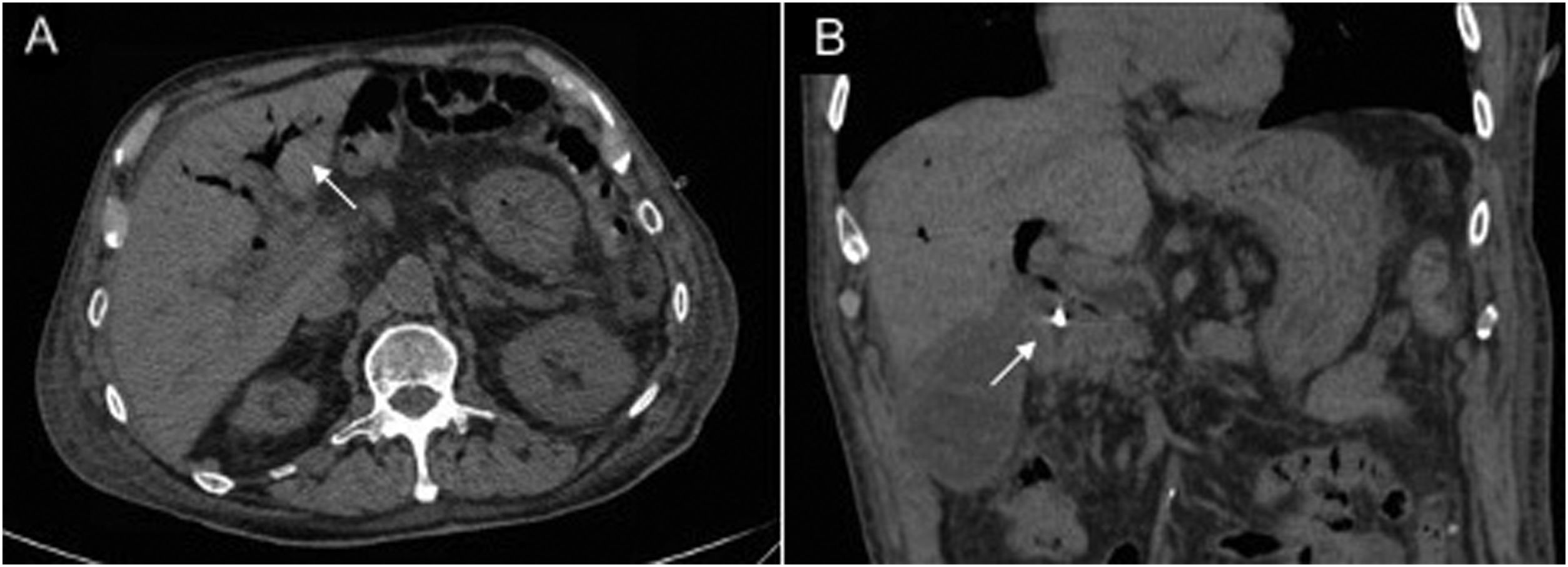
An 84-year-old man was admitted to the accident and emergency department due to signs and symptoms of haematemesis, haemodynamic instability and transfusion requirement. Following volume replacement therapy, early gastroscopy was performed, revealing an ulcer on the anterior aspect of the duodenal bulb with spurting blood, which was treated by placing an endoclip and breaking up the fibrinous area. The examination was complemented with an emergency abdominal CT scan which showed pneumobilia in the intrahepatic biliary tract and common bile duct, as well as an air-fluid level in the gallbladder; these findings were consistent with a fistula between the duodenal ulcer and the biliary tract. Conservative treatment was agreed upon with the surgery department, given the patient's comorbidity and lack of abnormal laboratory test results (Figs. 1–2).
 Partially fibrinous ulcer in the duodenal bulb, with a visible pulsatile vessel and a haemostasis clip. B) Follow-up endoscopy at 12 weeks: clear outflow of bile through the fistula opening on a fibrinous duodenal ulcer.")
 Presence of pneumobilia in the intrahepatic biliary tract. B) Pneumobilia in the intrahepatic biliary tract and common bile duct and metal clip in the area of the duodenal bulb, findings suggestive of a duodenal biliary fistula.")
A bilioenteric fistula is an abnormal connection between the biliary tract and the gastrointestinal tract. It may develop after surgery or spontaneously in the context of biliary disease. More rarely, this type of fistula develops as a complication of peptic ulcer disease.1
The clinical picture ranges from no symptoms to symptoms particular to peptic or biliary ulcer disease. In asymptomatic cases, diagnosis is usually incidental in the course of endoscopic or radiological examination. Pneumobilia in the absence of biliary tract manipulation suggests this complication as a possible diagnosis.2
Treatment is usually surgical with fistula resection and perforation repair. However, it should be personalised depending on the patient's clinical situation and comorbidity: in some cases, a combination of medical and endoscopic treatment is sufficient to achieve ulcer healing.3
FundingNo funding was received for this study.
Please cite this article as: Aparicio Serrano A, González Galilea Á, Rodríguez Tirado MI, Jurado García J. Fístula duodeno-biliar: una complicación infrecuente de una úlcera duodenal. Gastroenterol Hepatol. 2022;45:293–294.
