



An 84-year-old male was referred to the emergency service with a history of fever, dysuria and polyuria with a duration of 2 days. There was also a complaint of discrete asthenia and a recent high-grade glioblastoma excision under post-intervention corticosteroid therapy (dexamethasone 4mg once daily).
Initially admitted with suspicion of nosocomial infection, it was empirically treated with piperacillin/tazobactam with posterior confirmation of urinary tract infection by positive culture for Enterococcus faecalis and Serratia marcescens, the latter also as bacteriemia. Therapy was adjusted to a directed course of ciprofloxacin and vancomycin as indicated by sensitivity results, with initial clinical improvement after 10 days.
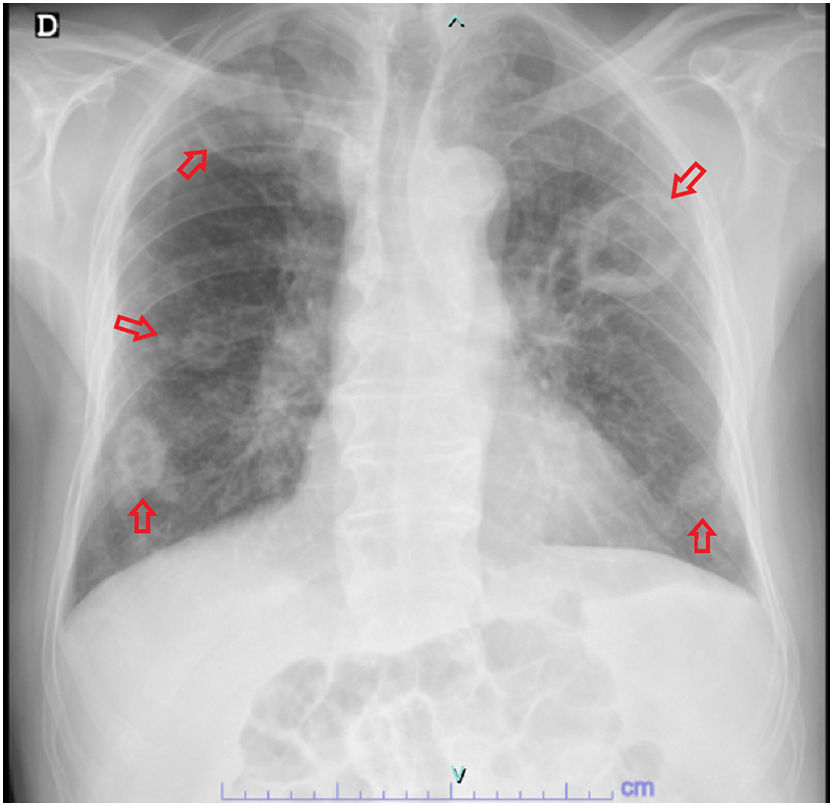
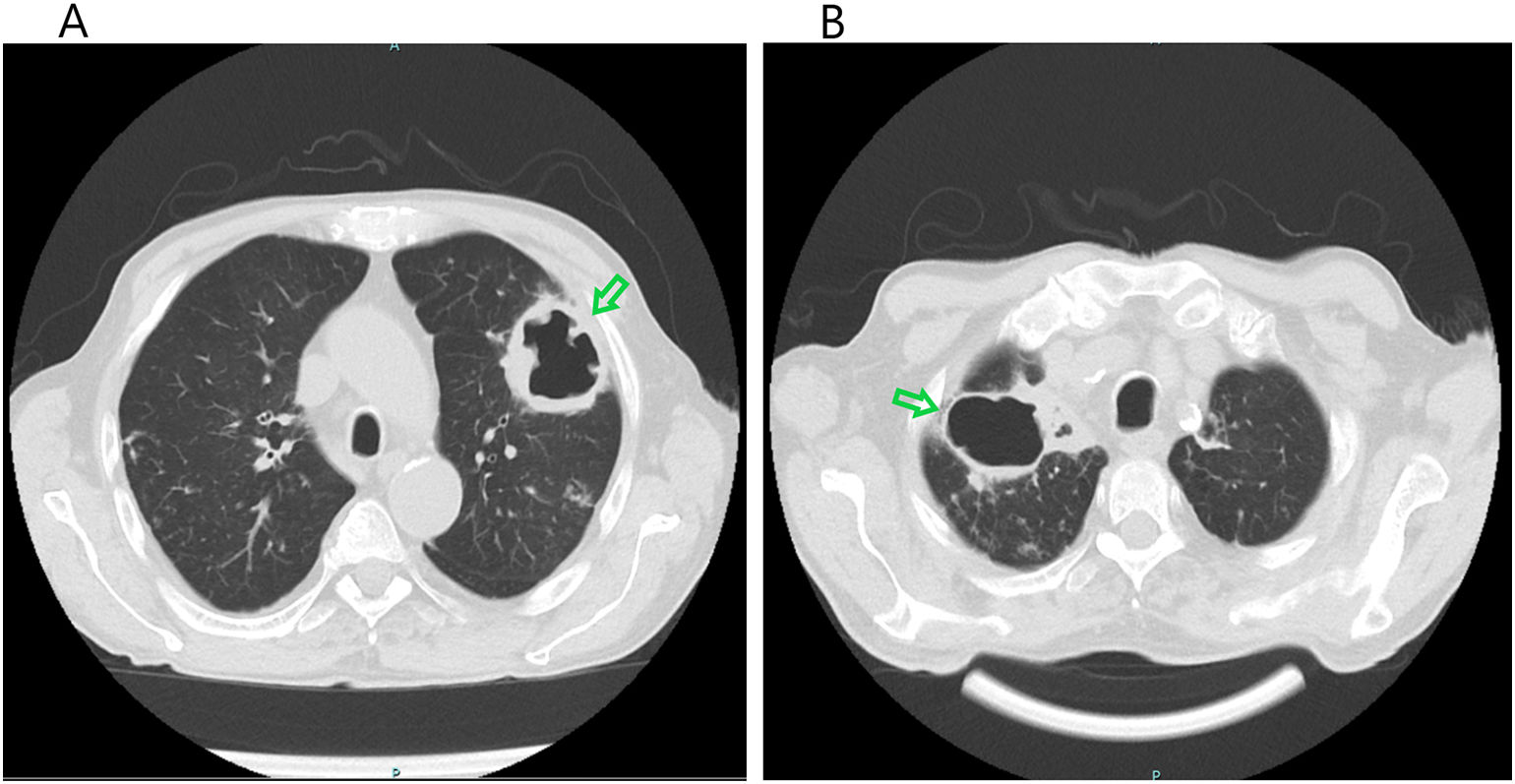
Under this antibiotic course, the patient started developing dyspnoea, a productive cough with hemoptoic sputum and reappearance of fever. Sputum culture isolated the same strain of Serratia already identified and chest radiography demonstrated new pulmonary nodular bilateral lesions (Fig 1), confirmed to be of de novo pulmonary abscesses on chest CT scan (Fig 2A and 2B).
, not present on admission.")
 demonstrating the larger lesions visible on the chest radiography (green arrow), corresponding to cavitated abscess of 67mm in the right apical lobe and a 54mm diameter lesion localized in the posterior segment of the left superior lobe.")
Immunocompromised patients, even under directed therapy, may have inadequate response rates and are at greater risk of infectious complications, in this case, hematogenous dissemination from a urinary starting point to multiple lung abscesses of significant size, requiring readjustment of antibiotic therapy to 6 weeks of meropenem, with favourable response.
