


To determine the relationship between postcircumcisional mucosal cuff length due to performance of circumcision and premature ejaculation (PE).
Materials and methods180 circumcised men were enrolled in the study, including 60 men with PE circumcision performed by doctors (Group 1), 60 men with PE circumcision performed by non-medical personnel (Group 2) and 60 men without PE. Data considered for analysis consisted of age, circumcision age, education, smoking, penile length, mucosal cuff, penile skin lengths and Intravaginal Ejaculation Latency Time (IELT).
ResultsThe mean age of study group was 32.7±10.4 (range 24–56). The mean of IELT was 0.6±0.1min (min) in group 1, 0.5±0.1min in Group 2 and 4.3±0.3min in healthy group. The mean of penis length was 123.2±12.8mm in group 1, 124.6±11.7mm in group 2 and 124.8±13.4mm in healthy group. The mean of penile mucosa was 11.7±1.7mm in group 1, 14.8±3.1mm in group 2 and 12.8±3.1mm in healthy group. There was no difference between the three groups regarding the length of the penile mucosal cuff (p=0.89). Patients circumcised by doctors in group 1 had significantly shorter postcircumcisional mucosal cuff length than group 2 patients circumcised by personnel except doctors (p=0.42); but there was no statistical difference in IELT between group 1 and group 2.
ConclusionsThe result of this study is that circumcisions performed by doctors have shorter mucosal cuff but the length of mucosa is not a risk factor in premature ejaculation.
Determinar la relación entre la longitud del manguito de la mucosa secundario a circuncisión y la eyaculación precoz (EP).
Material y métodos180 hombres circuncidados y con EP fueron incluidos en este estudio, de los cuales 60 fueron circuncidados por médicos (grupo 1) y 60 por personal no-médico (grupo 2); también fueron incluidos 60 pacientes sin EP. Datos recogidos para el análisis fueron la edad del paciente en el momento del análisis, la edad en la que se realizo al circuncisión, educación, habito tabáquico, las longitudes del pene, del manguito de la mucosa y de la piel del pene; y la latencia de eyaculación intravaginal (LEIV).
ResultadosLa media de edad de los pacientes era de 32.7±10.4 años (rango 24-56). La media de LEIV era 0.6±0.1 minutos (min) en el grupo 1; 0.5±0.1min en el grupo 2 y 4.3±0.3min en el grupo sano. La media de la longitud del pene era 123.2±12.8mm en el grupo 1, 124.6±11.7mm en el grupo 2 y 124.8±13.4mm en el grupo sano. La media de la mucosa peneana era 11.7±1.7mm en el grupo 1, 14.8±3.1mm en el grupo 2 y 12.8±3.1mm en el grupo sano. No había diferencias entre los grupos respecto la longitud del manguito de la mucosa (p=0.89). Los pacientes del grupo 1 tenían el manguito de la mucosa del pene más corta que los pacientes del grupo 2 que fueron circuncidados por personal no-médico (p=0.42), pero no había diferencias estadísticamente significativas en cuanto a LEIV entre grupos.
ConclusionesEl manguito de la mucosa del pene es más corta si se realiza por médicos, pero la longitud de la mucosa no es un factor de riego para la eyaculación precoz.
Premature ejaculation (PE) is one of the most prevalent sexual complaint of men, affecting about one of three men.1 In the past 5 years, there has been a remarkable upsurge in interest and research activities concerning PE, which previously was compared to erectile dysfunction (ED).2 Although some psycological, organic and sociocultural factors have been proposed to cause PE, the exact pathogenesis of PE remains to be clarified.3 One of the conflicting factor is the effect of postcircumcisional mucosal cuff length on ejaculation and also there are some concerns about leaving so much mucosa by the performer of the circumcision.4–9 Circumcision is routinely performed in Jewish and Muslim culture. Twenty percent of all men worldwide are considered to be circumcised and this ratio may vary in different countries.10 We examined the relationship between postcircumcisional mucosal cuff length due to performance of circumcision and PE.
Materials and methodsThe study was a single centre, retrospective study that was approved by the local ethics committee and all participants provided signed informed consent. From November 2012 to December 2013, all men with the complaint of lifelong PE who came to our clinic (Ankara Training and Research Hospital) were investigated. Totally 221 volunteers aged from 24 to 56 years enrolled in the study. Patients with a history of sexual dysfunction(s) caused by other conditions that are known to cause erectile dysfunction, such as sympatholytic drug use or diabetes mellitus, ejaculatory dysfunction, such as prostatitis or multiple sclerosis, having received drug therapy that may affect ejaculation time, who were uncircumcised or having lower urinary tract symptoms were excluded from the study. Almost all contributors had sexual intercourse 1–2 times per week. Circumcised men with intravaginal ejaculation latency time (IELT) of less than 60seconds were considered to have PE.11 IELT was defined as the time between start of vaginal intromission and the start of intravaginal ejaculation. Stopwatch measurements were performed by patient partners to measure IELT. Patients were asked to make stopwatch recordings at least 5 times. All patients with PE met the criteria of the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV-TR®). History, physical examination (circumcision status) and measurements of penile skin length (PSL), penile mucosal cuff length (MCL) and stretched penile length (PL) were performed by one surgeon.
Statistical analysisResults are expressed as the mean±SD. The variables were investigated using the visual (histograms probability plots) and analytical methods (Kolmogorov–Simirnov test) to determine whether or not they are normally distributed. Chi-square, Fisher's exact test, and independent samples test were used for comparison of variables between the groups. All statistical analyses were performed using SPSS ver.16.5 (Statistical Package for social Sciences for Windows 16.5 Inc., Chicago, IL, USA). A p value of less than 0.05 was set as statistically significant.
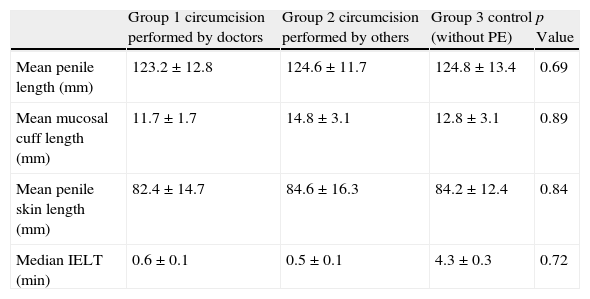
ResultsForty-one patients were excluded from the study according to exclusion criteria and initially 180 circumcised men were included in the study, including 60 men with PE who had circumcision performed by doctors (Group1), 60 men with PE who had circumcision performed by personnel except doctors (Group 2) and 60 men as the control group who were age-matched men without PE. The mean age of study group was 32.7±10.4 years. Sexual characteristics of the circumcised men with PE (subdivided into two groups according to performance of circumcision) and men in the control group are summarized in Table 1. The mean of IELT was 0.6±0.1minutes (min) in group 1, 0.5±0.1min in Group 2 and 4.3±0.3min in healthy group. The mean of penis length was 123.2±12.8mm in group 1, 124.6±11.7mm in group 2 and 124.8±13.4mm in healthy group. The mean of penile mucosa was 11.7±1.7mm in group 1, 14.8±3.1mm in group 2 and 12.8±3.1mm in healthy group. There was no difference between the three groups regarding the length of the penile mucosal cuff (p=0.89). Patients circumcised by doctors in group 1 had significantly shorter postcircumcisional mucosal cuff length than group 2 patients circumcised by personnel except doctors (p=0.42) but there was no statistical difference in IELT between group 1 and group 2.
Sexual characteristics of circumcised men with PE and control group.
| Group 1 circumcision performed by doctors | Group 2 circumcision performed by others | Group 3 control (without PE) | p Value | |
| Mean penile length (mm) | 123.2±12.8 | 124.6±11.7 | 124.8±13.4 | 0.69 |
| Mean mucosal cuff length (mm) | 11.7±1.7 | 14.8±3.1 | 12.8±3.1 | 0.89 |
| Mean penile skin length (mm) | 82.4±14.7 | 84.6±16.3 | 84.2±12.4 | 0.84 |
| Median IELT (min) | 0.6±0.1 | 0.5±0.1 | 4.3±0.3 | 0.72 |
As the most common male sexual disorder, PE affects 30–40% of sexually active men, and up to 75% of men will experience at least one episode of PE at some point in their lifetime.12 Despite the high prevalence of PE, its etiology is unclear in most cases although it is increasingly accepted that PE may result from organic or psychogenic causes.13 Male circumcision is one of the concerning factor that may affect PE.5,6
Male circumcision has been performed for over 15,000 years and remains one of the most common operations in the world.14,15 20% of all men worldwide are thought to be circumcised and it is reported to be 48% in Canada, 24% in England, and 82% white men and 54% African American men in the USA.8,10 Although circumcision provides improved penile hygiene and protects against HIV and other sexually transmitted diseases, controversies emerged about true role of circumcision on penile sensibility and sexual satisfaction.15–17 There are conflicting studies regarding the effect of circumcision on IELT. Some reported increased and some reported decreased sensitivity, and still others reported variable penile sensitivity with their own proposed mechanism and role for foreskin.18 Also, there are concerns regarding the length of mucosal cuff after circumcision and its effect on IELT later in life.
Majority of studies show no difference or improvement in sexual function, sensitivity and satisfaction after circumcision. In a study of Hosseini et al. 84 circumcised men, including 42 men with PE and 42 without, were investigated and between the two groups, no statistically significant differences in IELT were seen that could be correlated with any length of penile, mucosal cuff and penile skin measurements.7 In contrast, Senel et al. examined the long-term effects of circumcision on sexual function and concluded that circumcision did not adversely affect sexual functions, but it caused a significant improvement in erectile function and overall sexual satisfaction.19 In another study by Zhang et al., 52 cases suffering from PE and possessing a redundant prepuce were treated with circumcision and they found a relationship between a redundant prepuce and PE, so that circumcision was an effective method to treat PE.20 The mucosal cuffs left by physicians were shorter than the others, probably as a result of the doctor's choice of surgical technique while others use the one-cut clamp technique, and perhaps the surgical technique leaves a shorter mucosal cuff.8
To conclude, according to the theory that men with a larger mucosal cuff have a higher chance of experiencing PE due to performance of circumcision by a doctor or not, we have not found any relationship between postcircumcision mucosal cuff length and PE. But postcircumcisional mucosa was shorter in circumcision operated by doctors. Also, there were no relationships between penile length, penile skin length, smoking, education, circumcision timing, and PE.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work centre on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestNone of the authors have any conflicts of interest related to this study.