


The mean platelet volume (MPV) has important role in the pathophysiology of vascular diseases as a marker of the platelet activity. To investigate the association between mean platelet volume and erectile dysfunction (ED) and to search whether this marker can be used for diagnosis of ED.
Materials and methodsOf the 312 patients with ED of various degrees, 122 patients without ED (IIEF-5>21) were included in this prospective study. Severity of ED was determined according to IIEF-5 questionnaire. MPV, fasting serum glucose, cholesterol, low density lipoprotein (LDL) and serum testosterone levels are also recorded. The mean platelet volume was calculated by the Coulter counter technique and sexual function was determined by International Index of Erectile Function erectile function domain (IIEF-5).
ResultsThe mean age of patients was 58.4 years. The mean MPV value of patients with ED was significantly higher compared to the non-ED patients (8.91 vs. 8.22, p=0.0001). The severity of ED was shown to have a positive strong correlation with MPV values (r=0.719, p=0.001). Mean serum triglyceride, glucose, total cholesterol and LDL cholesterol levels were noted higher in patients with ED. MPV values were found to be significantly higher in patients with ED.
ConclusionMPV level shows significant correlation with severity of ED. This cheap laboratory test can have potential to be a marker of ED. Further prospective larger studies with vascular wall thickness measurements should be conducted.
El volumen plaquetario medio (VPM) desempeña un papel importante en la fisiopatología de las enfermedades vasculares como marcador de la actividad plaquetaria. El objetivo fue investigar la asociación entre el VPM y la disfunción eréctil (DE), y averiguar si este marcador puede utilizarse para el diagnóstico de la DE.
Materiales y métodosDe los 312 pacientes con disfunción eréctil de diversos grados, 122 pacientes sin disfunción eréctil (Índice Internacional de la Función Eréctil [IIEF-5]>21) se incluyeron en este estudio prospectivo. La gravedad de la DE se determinó según el cuestionario IIEF-5. También se analizaron el VPM, la glucosa sérica, el colesterol, la lipoproteína de baja densidad (LDL) y los niveles séricos de testosterona. El volumen plaquetario medio se calculó mediante la técnica de contador Coulter y la función sexual se estableció mediante el dominio de la función eréctil del IIEF-5.
ResultadosLa media de edad de los pacientes fue de 58,4 años. El valor medio del VPM de los pacientes con DE fue considerablemente mayor en comparación con los pacientes sin DE (8,91 frente a 8,22; p=0,0001). La gravedad de la DE mostró una fuerte correlación positiva con los valores de VPM (r=0,719; p=0,001). Los niveles séricos de triglicéridos, glucosa, colesterol total y colesterol-LDL fueron más altos en pacientes con DE. Los valores del VPM se encontraron considerablemente mayores en pacientes con DE.
ConclusiónEl nivel del VPM muestra una correlación importante con la gravedad de la DE. Esta prueba de laboratorio barata puede tener el potencial de ser un marcador de DE. Se deben realizar más estudios prospectivos más grandes con mediciones del espesor de la pared vascular.
Erectile dysfunction (ED) has been defined as the persistent inability to attain and maintain an erection sufficient to permit satisfactory sexual performance.1 Although prevalence of ED is estimated to be 19–52% in general population, it is found higher rate (44–65%) in cardiovascular disease patients.2–4 As cardiovascular disease and ED overlap in risk factors, prevalence and manifestation, they are thought to share both the etiology of and progression of the disease process. Common risk factors of both conditions include aging, atherosclerosis, diabetes mellitus (DM), hypertension (HT), smoking and dyslipidemia. All of these risk factors are associated with endothelial dysfunction.5,6
Vascular pathologies may result in changes in blood elements. Platelet activation is seen in common vascular pathologies such as coronary atherosclerosis, myocardial infarction, and stroke.7,8 Increase in mean platelet volume (MPV) is a determinant of platelet activation therefore it may have a role in early detection of vascular pathologies. It is also associated with risk factors of endothelial dysfunction such as diabetes, hypertension, obesity and smoking.9–11
The association between endothelial dysfunction and ED together with shared risk factors raise the importance of markers for early detection of vascular dysfunction. MPV a cheap and valuable marker of platelet activation can be a candidate for early detection of vascular ED. Very limited reports have studied MPV in the patients with erectile dysfunction, which have demonstrated relationship between MPV and ED.12,13 To our knowledge, this is the largest series to assess the association between MPV and ED. We aimed to evaluate and compare the largest series of MPV value of patients with ED to control group of without ED.
Materials and methodsIn this prospective case control study totally 434 patients were included. The study group consisted of 312 male patients that applied to outpatient clinics of Ufuk University and Ankara University Urology departments with complaint of ED between March 2012 and September 2012 and 122 age-matched male patients, admitted to the outpatient clinics with non-ED complaints (stone disease, flank pain, etc.) and IIEF-5 score >21 were involved as control group. All patients signed informed consent form.
Patient evaluationAll patients underwent complete physical examination for any sign of hypogonadism, penile deformities and all patients filled the IIEF-5 for investigation of presence and severity of ED. Platelet count (nPLT) and MPV measurement were also recorded for all patients.
Laboratory analysisAfter an overnight fasting period, two blood samples were taken from each patient from antecubital vein in the morning (8am–10am) and the samples were collected into tubes including dipotassium ethylenediaminetetraacetic acid (EDTA). The mean of the two values is recorded for analysis. To prevent in vitro platelet activation, the measurements were performed within 1 hour after sampling. Platelet counts and MPVs were obtained by the Coulter counter technique (Coulter Gen.S® Hematology Analyzer, Beckman Coulter Corp, Hialeah, FL, USA). Fasting serum glucose, cholesterol, low density lipoprotein and serum testosterone levels were also recorded. For measurement of testosterone, chemiluminescent method and Advia Siemens Centaur kits (Siemens Healthcare Diagnostic Inc., Malvern, Pennsylvania, USA) was used.
The severity of ED was classified as: severe (5–7), moderate (8–11), mild to moderate (12–16), mild (17–21), and no ED (22–25). History of DM and smoking together with body mass index were also recorded. History of smoking was especially investigated as it was shown to increase MPV levels.14
Inclusion criteria- 1.
50–70 years old male patients. 2. Normal libido. 3. No previous use of PDE5 Is. 4. Normal Serum testosterone levels (>300ng/ml).
- 1.
History of any pelvic surgery. 2. Having any kind of medication for ED. 3. History of diagnosis for cerebrovascular disease or symptomatic cardiovascular disease. 4. History of any medication or surgery for cardiovascular disease. 5. History of antiaggregant or anticoagulant medication. 6. Malignancy. 7. Infectious diseases. 8. Neurogenic or endocrinological ED primary study outcome was the value of MPV on determination ED and its correlation with severity of ED.
Power analysis is performed and to determine the effect size MPV values were expected to be between 8 and 10. A difference of 0.2 points (10% difference) was accepted as effect size and with power level of 80% the analysis revealed that at least 60 patients should be included in each group.
Statistical analysisFor statistical analysis SPSS 17.0 (SPSS, Inc., Chicago, IL) software was used. Normal distribution was tested with Kolmogorov–Smirnov test. Data is expressed as numbers and percentages for discrete variables and as means±SD for continuous variables. The chi-square analysis or Fishers exact test was used to assess the significance of differences between dichomatous variables. Continuous variables were compared by Student's t test or Mann–Whitney U test. Spearman's correlation analysis is performed to detect correlation between MPV and severity of ED and serum cholesterol and LDL levels. Logistic regression analysis was performed to determine the effect of MPV measurement as an independent predictor of developing ED, age, DM, smoking, hypercholesterolemia and BMI>30 were included in the analysis as other risk factors. p value of 0.05 was accepted for statistical significance.
ResultsMean age of all population was 58.4 years and DM was present in 143 patients (32.9%). The percentage of diabetic patients was higher in patients with ED compared to non-ED patients, however, the difference was not statistically significant (34.9% vs. 27.8%, p=0.142). Severe ED was detected in 62 patients, moderate ED was detected in 78 patients; mild to moderate ED was detected in 80 patients and mild ED was detected in 92 patients.
The MPV value of patients with ED was significantly higher compared to the non-ED patients (8.91 vs. 8.22, p 0.0001). Additionally the severity of ED was shown to have a positive strong correlation with MPV values (r=0.719, p=0.001). Also serum cholesterol levels (r=0.552, p=0.01) and LDL levels (r=0.558, p=0.01) were found to have positive moderate correlation with MPV values. Mean MPV values of subgroups of ED were as follows; severe ED: 9.53, moderate ED: 9.29, mild to moderate ED: 8.68, mild ED 8.38. The difference between both groups was significant and values are summarized for subgroups in Table 1.
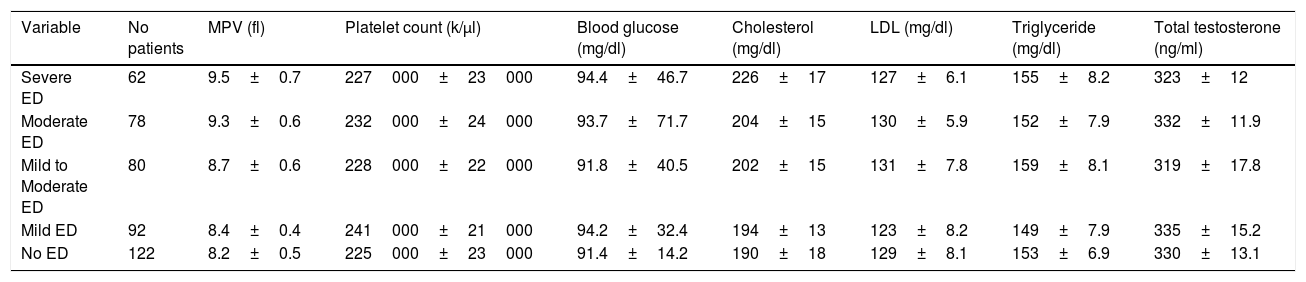
The mean serum levels of studied parameters of the groups based on ED severity.
| Variable | No patients | MPV (fl) | Platelet count (k/μl) | Blood glucose (mg/dl) | Cholesterol (mg/dl) | LDL (mg/dl) | Triglyceride (mg/dl) | Total testosterone (ng/ml) |
|---|---|---|---|---|---|---|---|---|
| Severe ED | 62 | 9.5±0.7 | 227000±23000 | 94.4±46.7 | 226±17 | 127±6.1 | 155±8.2 | 323±12 |
| Moderate ED | 78 | 9.3±0.6 | 232000±24000 | 93.7±71.7 | 204±15 | 130±5.9 | 152±7.9 | 332±11.9 |
| Mild to Moderate ED | 80 | 8.7±0.6 | 228000±22000 | 91.8±40.5 | 202±15 | 131±7.8 | 159±8.1 | 319±17.8 |
| Mild ED | 92 | 8.4±0.4 | 241000±21000 | 94.2±32.4 | 194±13 | 123±8.2 | 149±7.9 | 335±15.2 |
| No ED | 122 | 8.2±0.5 | 225000±23000 | 91.4±14.2 | 190±18 | 129±8.1 | 153±6.9 | 330±13.1 |
Values are shown as the mean±standard deviation. Coefficients of variation values of MPV were 0.05–0.07. The MPV value of patients with ED was significantly higher compared to the non-ED patients (8.91 vs. 8.22, p=0.0001). Severity of ED was shown to have a positive strong correlation with MPV values (r=0.719, p=0.001).
Mean platelet count of the groups did not show significant difference. Patients with ED were shown to have higher mean serum cholesterol, LDL cholesterol, triglyceride and glucose levels compared to the non-ED patients. However the difference of mean total testosterone levels were not found to be different (p=0.129). Percentage of smoking patients was found to be higher in the moderate and severe ED groups. Percentage of patients with BMI>30 was also higher in the moderate and severe ED groups. The values of these serum parameters are summarized in Table 1.
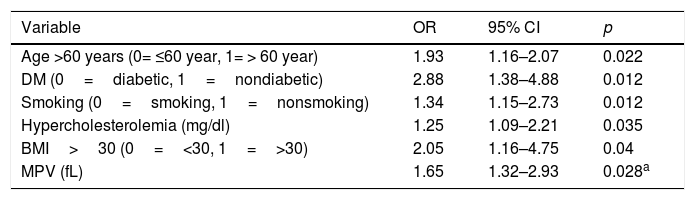
When binary logistic regression analysis was performed, age, DM, hypercholesterolemia, BMI, smoking and MPV values were found to be independent risk factors for development of ED. The results of binary logistic regression analysis are summarized in Table 2.
Logistic regression analysis for factors of development of ED.
| Variable | OR | 95% CI | p |
|---|---|---|---|
| Age >60 years (0= ≤60 year, 1= > 60 year) | 1.93 | 1.16–2.07 | 0.022 |
| DM (0=diabetic, 1=nondiabetic) | 2.88 | 1.38–4.88 | 0.012 |
| Smoking (0=smoking, 1=nonsmoking) | 1.34 | 1.15–2.73 | 0.012 |
| Hypercholesterolemia (mg/dl) | 1.25 | 1.09–2.21 | 0.035 |
| BMI>30 (0=<30, 1=>30) | 2.05 | 1.16–4.75 | 0.04 |
| MPV (fL) | 1.65 | 1.32–2.93 | 0.028a |
ED is a multifactorial disease that causes significant decreases in quality of life of both patients and their partners.2 The most common cause of ED in aging male is vascular pathology due to atherosclerosis.6,15
Penile erection is a complex procedure resulting from coordinated work up of vascular, neuronal and psychosomatic systems. Endothelial cells are the main source of nitric oxide (NO) that is responsible for regulation of vascular function. Endothelial dysfunction results in decrease in levels of NO. NO not only regulates the vascular tonus but also inhibits the platelet activation. Free oxygen radicals result in adhesion of white blood cells and platelet adhesion. This causes release of vasoconstrictive substances, which further results in platelet aggregation.16,17
ED and cardiovascular diseases share common risk factors. These risk factors result in endothelial dysfunction, which is the main pathophysiologic mechanism of both conditions. Clinical trials showed that ED occurs 2–5 years before cardiovascular disease.18,19 This is mainly due to anatomical reasons that is the vascular diameter of penile artery (1–2mm) is much less than coronary arteries (3–4mm). Plaque size that causes ED, results in 30–40% obstruction in coronary arteries and the study by Montorsi et al. showed that 67% of males with ED develop anginal symptoms in 3 years period.18 Blumentals et al. concluded that ED can be a marker for acute myocardial infarction.20
Platelet aggregation and its association with vascular wall have importance in pathogenesis of atherosclerosis and its complications. Proatherogenic effect of platelet activity is the main cause of atherosclerosis and cardiovascular disease. Current studies showed that acute myocardial infarction, unstable angina pectoris and ischemic heart disease are associated with increased platelet volume. Therefore this mechanism has the potential to be important in pathogenesis of ED and MPV is a candidate for screening of ED.21,22
A few reports have studied MPV in the patients with erectile dysfunction. Ciftci et al. have demonstrated that the MPV and platelet values were significantly higher in 50 patients with vasculogenic ED.12 They have found that the MPV values were not statistically significantly different between in the patients with severe ED and mild ED (p>0.05). Aldemir et al. have evaluated blood total platelet count, MPV and platelet distribution width (PDW) values of patients with ED and control group.13 They have shown that MPV and PDW values significantly increased in patients with ED compared with the control group. However, both above reports have studied on small cohort with ED. Furthermore, their outcomes were not specifically evaluated for correlation with MPV and patients with ED.
Up to our knowledge, our study is the largest trial to investigate the role of MPV on erectile function. Our results show that mean MPV value has significant correlation with ED presence and severity. The MPV was found to be different even between severe and moderate ED. None of the patients had sign of hypogonadism and serum testosterone levels were normal, therefore the results reflect the population that is generally encountered in daily practice.
Presence of DM was slightly higher in patients with ED. This may be associated with increased levels of MPV and this may also result in increased efficacy of MPV on detection of vascular ED.
Some studies have demonstrated a relationship between MPV with smoking, diabetes dyslipidemia and age.9–11,23 Some researchers excluded these factors to evaluate the MPV in their studies.12,23 Although we did not exclude these factors, we used logistic regression analysis to minimize the effect of these variables on MPV values.
The most important drawback of our study is lacking objective measurements for clinical significance of ED, such as carotid artery intima media thickness, penile duplex testing and nocturnal penile tumesance. Results of these studies would prove the endothelial damage and clinical significance of ED and explain the association between ED and MPV. However this is a preliminary study and further studies with vascular wall thickness measurement should be conducted. Additionally serum estradiol levels have not been measured which would participate in degree of ED and should better be included in logistic regression analysis.
ConclusionMPV values are found to be significantly higher in patients with ED, and MPV level shows significant correlation with severity of ED. This cheap laboratory test may have potential to be a marker of ED.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestThere is no conflict of interest.