









Social anxiety has been widely studied over the past four decades. However, limited attention has been given to the relationship between social anxiety and interpersonal difficulties during adolescence. Adolescents exhibiting symptoms of social anxiety (SA) may also face challenges in their interpersonal interactions at school. This study aimed to identify distinct profiles of adolescents with social anxiety and examine whether these profiles differed in terms of the severity of their interpersonal difficulties (ID). A random cluster sampling was performed. The sample comprised 1,685 Spanish students (49.0% female) from 15 to 18 years old (M = 16.28, SD = 0.97). Participants completed the Spanish version of the Social Anxiety Scale for Adolescents (SAS-A) and the Questionnaire About Interpersonal Difficulties for Adolescents (QIDA). Latent Profile Analysis (LPA) revealed four social anxiety profiles: mild SA, moderate SA, severe SA, and extreme SA. Multivariate analyses (MANOVA) indicated statistically significant differences in interpersonal difficulties across the four clusters with effect sizes between d = 0.23 and d = 0.91. The mild SA profile showed the lowest mean scores in interpersonal difficulties whereas the extreme SA profile showed the highest ones. Intervention strategies are suggested as preventive or corrective measures to support adolescents who fall in high-risk profiles.
La ansiedad social ha sido ampliamente estudiada en las últimas cuatro décadas. Sin embargo, se ha prestado escasa atención a la relación entre la ansiedad social y las dificultades interpersonales durante la adolescencia. Los adolescentes que presentan síntomas de ansiedad social (AS) también se enfrentan a desafíos en sus interacciones interpersonales en la escuela. Este estudio tiene como objetivo identificar los distintos perfiles de adolescentes con ansiedad social y examinar si difieren en cuanto a la gravedad de sus dificultades interpersonales (DI). Se ha realizado un muestreo aleatorio por conglomerados. La muestra incluye 1685 estudiantes españoles (49.0% chicas) de 15 a 18 años (M = 16.28, DT = 0.97). Los participantes han completado la versión en español de la Social Anxiety Scale for Adolescents (SAS-A) y el Questionnaire About Interpersonal Difficulties for Adolescents (QIDA). El Análisis de Perfiles Latentes (LPA) revela cuatro perfiles de ansiedad social: AS leve, AS moderada, AS grave y AS extrema. Los análisis multivariados (MANOVA) indican diferencias estadísticamente significativas en dificultades interpersonales entre los cuatro grupos, con tamaños del efecto entre d = 0.23 y d = 0.91. El perfil de AS leve presenta las puntuaciones medias más bajas en dificultades interpersonales, mientras que el perfil de AS extrema presenta las más altas. Se sugieren estrategias de intervención como medidas preventivas o correctivas para apoyar a los adolescentes que presentan perfiles de alto riesgo.
Adolescents are a vulnerable population susceptible to experiencing internalizing problems, such as social anxiety (Esbjørn et al., 2010). Previous studies conducted using samples of Spanish adolescents have revealed a similar pattern of results (e.g., García-López et al., 2001). Social anxiety is overall characterized by fear of negative evaluation in social situations, anticipation of such evaluation (Dou et al., 2023) and discomfort in social situations. Social anxiety disorder is defined by a persistent and intense fear or anxiety concerning social situations in which an individual might face scrutiny or potential embarrassment. Social interactions, such as conversations, meeting new people, being observed, or performing in front of others, often serve as triggers for this fear or anxiety. It is important to note that a significant number of individuals display symptoms of social anxiety, even if they do not meet all the diagnostic criteria specified by the DSM-5-TR (American Psychiatric Association, 2022). Individuals with social anxiety are afraid of displaying symptoms of anxiety that could lead to negative external evaluation. The presence of negative emotions has an impact on social relationships and leads to maladaptive social functioning (Gonzálvez et al., 2019). As a result, adolescents with social anxiety often avoid many social situations and experience intense distress and anxiety (Gómez-Ortiz et al., 2016). Some authors have identified three specific factors in social anxiety: fear of negative evaluation (FNE), social avoidance and distress-new (SAD-N), and social avoidance and distress-general (SAD-G). These factors can be assessed using the Social Anxiety Scale for Adolescents (SAS-A; La Greca & López, 1998). The most extreme level of social anxiety can be found in social anxiety disorder (SAD), previously known as social phobia, which is one of the most prevalent disorders among adolescents (Burstein et al., 2011; Dou et al., 2023; García-López et al., 2008; Ollendick & Hirshfeld-Becker, 2002). Individuals with SAD often face challenges to start and maintain relationships with others (Kashdan et al., 2007; Rodebaugh, 2009; Tonge et al., 2020), and may employ maladaptive strategies, particularly in close relationships, leading to interpersonal distress.
For the purpose of this study, interpersonal difficulties refer to persistent problems with assertiveness, public speaking, intimacy, and the formation and maintenance of relationships, such as in close friendships and heterosexual and family relationships. Although these difficulties may or may not stem from social anxiety, socially anxious individuals encounter difficulties in achieving mutual and emotional intimacy within relationships (Wenzel, 2001). Additionally, adolescents with social anxiety are inclined to develop negative perceptions of their relationships with opposite-sex partners (Delgado et al., 2013). Therefore, investigating the association between social anxiety and interpersonal difficulties is crucial for improving the school adjustment of adolescents who may be experiencing relationship problems and showing avoidance behaviors. In this line, Méndez et al. (2002) found that the most stressful interpersonal situations for Spanish adolescents were defending their rights as users, public speaking, and interacting with peers of the opposite sex. In this line, several studies with large samples ranging from 16 to 70 years and beyond identified that these dimensions are closely linked to social anxiety as basic and core dimensions (e.g., Caballo, Salazar, Irurtia et al., 2010; Caballo et al., 2012, 2015).
In the field of educational research, there is an increasing focus on social anxiety worldwide, mainly in relation to academic achievement and performance, school refusal, absenteeism, and school anxiety (e.g., Urbán et al., 2023). In this sense, feared situations for adolescents with social anxiety include speaking in front of authority figures, asking and answering questions, participating in class discussions, joining teams, interacting with peers during break times, and attending social events and informal gatherings (García-López et al., 2008; Inglés et al., 2001; Martel et al., 2022). Such difficulties contribute to impairment in school settings, including problematic peer and teacher relationships (Martel et al., 2022). Thus, subclinical social anxiety is a potential explanation for adolescents' interpersonal difficulties in school context (Delgado et al., 2019, Vilaplana-Pérez et al., 2020). Social anxiety is, therefore, a significant predictor of interpersonal difficulties (Kim & Bae, 2022; Tonge et al., 2020).
Furthermore, the subclinical social anxiety manifested during adolescence may have implications for individuals' current and future interpersonal relationships (Koçak & Önen, 2014). In this line, Inglés et al. (2001) proposed the complementary hypothesis that interpersonal difficulties are a risk factor for subclinical social anxiety. Feeling rejected or socially excluded provokes worry and social distress, leading adolescents to avoid interpersonal relationships and social interactions, and social anxiety tends to increase with interpersonal difficulties. Despite previous research on social anxiety and interpersonal difficulties among Spanish adolescents, more sophisticated data analyses should be performed regarding the co-occurrence of these two factors in this population. This research gap is significant, considering that an increase in interpersonal difficulties during secondary school can negatively impact on adolescents' school adjustment (Urbán et al., 2023).
Therefore, as social anxiety is considered a key factor that contributes to interpersonal difficulties, further research on social anxiety among Spanish adolescents is necessary to prevent interpersonal difficulties and mitigate negative consequences among them. To address these gaps, a latent profile analysis (LPA), which employs a person-centered approach to identify subgroups of adolescents (Bauer, 2022; Morales et al., 2021), is used in this study. The reason for this selection is that adolescents with social anxiety do not form a uniform group and LPA assumes population heterogeneity (Spurk et al., 2020). Therefore, the general objective of this study is to examine the potential profiles of social anxiety and the existence of statistically significant differences in interpersonal difficulties among Spanish adolescents enrolled in Secondary Education. The specific objectives were: (1) To examine the number of different profiles of social anxiety of Spanish adolescents enrolled in Secondary Education; (2) To stablish the differences in interpersonal difficulties among the identified social anxiety latent profiles; and (3) To examine which social anxiety profile among Spanish adolescents enrolled in Secondary Education has the highest risk of experiencing interpersonal difficulties.
To achieve this objective, the following hypotheses are formulated: Hypothesis 1: Based on previous research on social anxiety profiles in Spanish adolescents, it is expected that a four-profile solution will emerge; Hypothesis 2: Spanish adolescents with higher levels of social anxiety are expected to experience more interpersonal difficulties, mainly in the areas of assertiveness, relationships with peers of the opposite sex, and public speaking.
MethodParticipantsA random cluster sampling method was used to recruit participants from Alicante, a province in southeastern Spain. The province was geographically divided into five areas: north, south, east, west, and center. Ten secondary schools were randomly selected, out of private, subsidized, and state ones in both urban and rural locations. Additionally, four classrooms were randomly chosen from each of the selected secondary education centers.
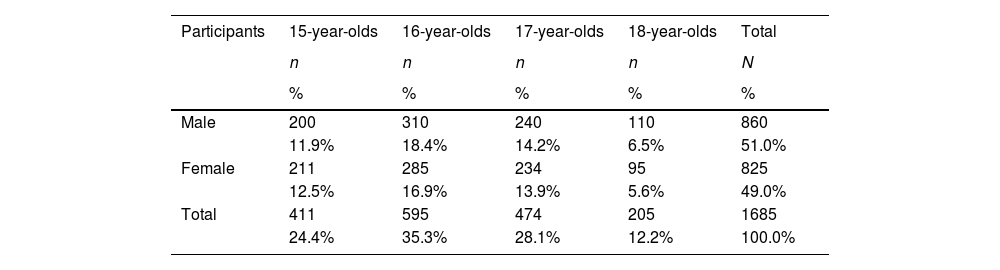
Initially, the sample consisted of 1,752 participants. 43 adolescents (2.45%) were excluded due to lack of written informed consent to participate in the study and 19 adolescents (1.08%) were excluded as they did not possess a proficient command of the Spanish language. Five adolescents (0.29%) decided to withdraw from the study. Participants did not gain any extra credits and were free to withdraw their participation at any time. Google Forms were used to administer the tests in order to avoid outliers and missing data, as an efficient method for data collection and management while minimizing the chances of data issues. Consequently, the final sample consisted of 1,685 adolescents, 49.0% female and 51.0% male. The age range of the participants was between 15 and 18 years, with a mean age of 16.28 (SD = 0.97). The distribution of the sample by age and gender is presented in Table 1.
Distribution of the sample by age and gender
| Participants | 15-year-olds | 16-year-olds | 17-year-olds | 18-year-olds | Total |
|---|---|---|---|---|---|
| n | n | n | n | N | |
| % | % | % | % | % | |
| Male | 200 | 310 | 240 | 110 | 860 |
| 11.9% | 18.4% | 14.2% | 6.5% | 51.0% | |
| Female | 211 | 285 | 234 | 95 | 825 |
| 12.5% | 16.9% | 13.9% | 5.6% | 49.0% | |
| Total | 411 | 595 | 474 | 205 | 1685 |
| 24.4% | 35.3% | 28.1% | 12.2% | 100.0% |
To assess the distribution of gender and age groups, Pearson's chi-square test of homogeneity was conducted. The analysis included eight groups, consisting of four age groups with two genders each. The results indicated that there were no statistically significant differences observed among the eight Gender x Age groups (χ2 = 1.79, p = .61).
InstrumentsSocial Anxiety Scale for Adolescents (SAS-A; La Greca & López, 1998). The Social Anxiety Scale for Adolescents (SAS-A) is a measurement tool used to evaluate adolescents' perceptions of their social anxiety. It consists of 18 self-statement items and four filler items that act as distractors. The 18 items are categorized into three subscales: fear of negative evaluation (FNE) which consists of eight items that focus on adolescents' concerns about negative evaluations by their peers; social avoidance and distress-new (SAD-N), with six items that examine social avoidance and distress in unfamiliar or new social situations; and social avoidance and distress-general (SAD-G) with four items that assess general social inhibition, distress, and discomfort. Participants rate each item on a 5-point Likert-type scale, ranging from 1 = not at all to 5 = all the time. The total SAS-A score ranges from 18 to 90, with higher scores indicating higher levels of social anxiety. Scores below 37 indicate “non-socially anxious” adolescents, while scores above 44 suggest the presence of social anxiety among adolescents (Olivares et al., 2002).
The SAS-A has versions in different languages, including Spanish (García-López et al., 2001), Portuguese (Cunha et al., 2004), Turkish (Aydin & Tekinsav-Sütçü, 2007), and Chinese (Zhou et al., 2008). In this study, the SAS-A Spanish version (García-López et al., 2001) was used. It presents high internal consistency, with Cronbach's alpha coefficients of .94 for FNE, .87 for SAD-N, .80 for SAD-G, and .91 for the total score. Additionally, Inglés et al. (2010) found measurement invariance for the correlated three-factor model of the SAS-A across gender and age samples. In this study, the reliability coefficients were as follows: Cronbach's alpha of .85 for FNE, .78 for SAD-N, and .75 for SAD-G; McDonald’s omega values of .87 for FNE, .79 for SAD-N, and .75 for SAD-G.
Questionnaire about Interpersonal Difficulties for Adolescents (QIDA; Inglés et al., 2005). The QIDA, also known as CEDIA in its Spanish version (Inglés et al., 2005), is a self-report measure consisting of 36 items divided into five subscales: assertiveness, heterosexual relationships, public speaking, family relationships, and close friendships. The assertiveness subscale (AS) has 16 items that assess anxiety related to making complaints, defending rights and interests, refusing unreasonable requests, and seeking information from individuals in daily life. The heterosexual relationships subscale (HR) consists of seven items focusing on perceived anxiety in interactions with the opposite sex. The public speaking subscale (PS) contains five items capturing anxiety when speaking in front of a large audience. The family relationships subscale (FR) includes four items addressing anxiety specifically related to assertiveness within the family context. The close friendships subscale (CF), the fifth and final subscale, consists of four items assessing anxiety associated with expressing gratitude, apologizing, and managing criticism from friends of both genders. Participants answer each item using a 5-point Likert scale, indicating the level of difficulty they experience in each situation and/or relationship, ranging from 0 = no difficulty to 4 = maximum difficulty.
Compared to other existing questionnaires, the QIDA provides a specific focus on situations that may arise interpersonal difficulties during adolescence (Caballo et al., 2018). Its applicability reaches beyond the Spanish-speaking population, as it has been translated and adapted into various languages, such as, Spain (Inglés et al., 2005), China (Inglés, Marzo et al., 2008), Iran (Shokri et al., 2010), Slovenia (Zupančič et al., 2011), France (Inglés et al., 2011), Colombia (Redondo et al., 2014), and Portugal (Inglés et al., 2022). In this study, the Spanish version of the QIDA, was used. The reliability coefficients for the subscales were as follows: Cronbach's alpha (α) of .91 for assertiveness, α = .88 for heterosexual relationships, α = .84 for public speaking, α = .76 for family relationships, and α = .71 for close friendships; and McDonald's omega coefficients were ω = .80 for assertiveness, ω = .88 for heterosexual relationships, ω = .77 for public speaking, ω = .72 for family relationships, and ω = .70 for close friendships. In a previous study by Inglés et al. (2005), a significant difference (effect size d = 1.53) was found in the total QIDA score among adolescents with and without subclinical social anxiety, as assessed by the Social Phobia and Anxiety Inventory. This finding supports the construct validity of the questionnaire, indicating that it accurately measures and differentiate adolescents based on their social anxiety status.
ProcedureFirst, to ensure transparency and cooperation, the purpose of this research was explained to the principals of each secondary education center, and their collaboration was requested. Written parental consents were collected over a two-week period. The questionnaires were then completed by the participants in the classroom during regular school hours. They were informed that the questionnaires were anonymous and voluntary. Google Forms were employed to ensure and maintain anonymity since data can be collected without directly linking adolescents to their specific responses, thus preserving their anonymity during the process. Furthermore, using Google Forms, the counterbalancing procedure was executed in order to avoid the bias of the order effect in the administration of the instruments. The average administration time was 20 minutes for the SAS-A and 30 minutes for the QIDA. A researcher was present in each classroom to provide instructions, address any concerns, and ensure that participants completed the scales independently.
This study followed the ethical standards of the Declaration of Helsinki of 1964 concerning research in human beings. It has also been conducted in accordance with the International Ethical Code in Humanities and Social Sciences of the Centre for Research Ethics & Bioethics. The study protocol was approved by the Ethics Committee of the University of Alicante, Spain, UA-2019-07-10. Written informed consent was obtained from the participants’ parents or legal guardians.
Data analysisFirstly, the associations between the dimensions of the Social Anxiety Scale for Adolescents (SAS-A) and the Questionnaire About Interpersonal Difficulties for Adolescents (QIDA) were examined by calculating Pearson correlation coefficients. Although Cohen’s d has a positive bias (Xiaofeng, 2023), Cohen's (1988) criterion was used for the interpretation of the coefficients: between 0.10 and 0.29, low correlation; between 0.30 and 0.49, moderate correlation; 0.50 or higher, strong correlation. Latent Profile Analysis (LPA) was used to compare different models (from 2 to 7 profiles) and determine the one that fits best. Prior to conducting the LPA, the scores derived from the three factors of the Social Anxiety Scale for Adolescents (SAS-A) were subjected to standardization. The standardized z-scores were then interpreted as follows: scores below -0.5 were indicative of low levels of social anxiety, scores between -0.5 and 0.5 indicated moderate levels, and scores above 0.5 denoted high levels of social anxiety.
In our study, we followed the general rule of considering multiple fit values, along with content decision criteria, when determining the final profile solution (Spurk et al., 2020). This process involved evaluating several indices and considering the theoretical interpretability of each model (Song & Kim, 2019). The Low Bayesian Information Criteria (BIC; Schwarz, 1978) and Akaike Information Criteria (AIC; Akaike, 1974) are two criteria for model selection. BIC considers model fit and complexity whereas AIC considers the likelihood of the model to predict future values. The Vuong-Lo-Mendell-Rubin Likelihood Ratio Test (Vuong, 1989; Lo et al., 2001) and the Bootstrap Likelihood Ratio Test (BLRT; McLachlan & Peel, 2000) are also used as fit indices for model selection. The LRT determines if a more complex model significantly improves the fit compared to a simpler one whereas the BLRT extends the LRT by using bootstrapping to estimate the null hypothesis distribution (Whittaker & Miller, 2020).
An optimal model is characterized by lower values of Low Bayesian Information Criteria (BIC) and Akaike Information Criteria (AIC), p ≤ .05 for both the Vuong-Lo-Mendell-Rubin Likelihood-Ratio Test (LRT) and the Bootstrap Likelihood Ratio Test (BLRT), and entropy scores close to 1. Additionally, each subgroup of participants was required to comprise at least 1% of the sample (Tein et al., 2013). Once the best model was established and with the purpose of checking if the proportion of males and females was similar in each cluster, the χ2 statistical was used.
After identifying the profiles of social anxiety, a multivariate analysis of variance (MANOVA) was conducted to examine the potential differences between these student groups in the mean scores of interpersonal difficulties. The variables met the assumptions of normality and homoscedasticity. The effect size was calculated and interpreted based on Cohen's d-values (1988), where values between 0.20 and 0.49, between 0.50 and 0.79, and above 0.80 represented small, medium, and large effect sizes, respectively. Data analysis was conducted using SPSS version 26 (IBM Corp, 2019) and MPlus version 8 software (Muthén & Muthén, 2017).
ResultsWith reference to the correlations among SAS-A and QIDA factors, there is a low correlation between fear of negative evaluation (FNE) and all QIDA factors. In the case of social avoidance and distress-new (SAD-N), there is a low correlation with public speaking, family relationships and close friendships, whereas there is a moderate correlation with assertiveness and heterosexual relationships. Regarding social avoidance and distress-general (SAD-G), despite a low correlation with heterosexual relationships, public speaking, family relationships and close friendships, there is a moderate correlation between SAD-G and assertiveness. The correlations among the total score of SAS-A and QIDA factors are generally low except for assertiveness, which exhibits a moderate correlation. These correlations are presented in Table 2.
Correlations among SAS-A and QIDA factors
| Variable | FNE | SAD-N | SAD-G | SAS_A |
|---|---|---|---|---|
| Assertiveness | .29* | .33* | .30* | .34* |
| heterosexual relationships | .18* | .33* | .28* | .29* |
| public speaking | .21* | .26* | .25* | .26* |
| family relationships | .17* | .19* | .17* | .20* |
| close friendships | .22* | .21* | .19* | .24* |
Note. FNE = fear of negative evaluation (FNE), SAD-N = social avoidance and distress-new, SAD-G = social avoidance and distress-general, SAS_A = total score.
The present study employs latent profile analysis to identify and determine different subgroups of participants based on their scores on the Social Anxiety Scale for Adolescents (SAS-A), which assessed fear of negative evaluation and social avoidance. We considered statistical criteria and interpretability of profiles to determine the best model. The goodness-of-fit indices for the estimated models are presented in Table 3.
Adjustment indices for latent profile models of social anxiety and interpersonal difficulties
| Models | AIC | BIC | BIC-adjusted | LRT p | LRT-adjusted | BLRT | Entropy | d |
|---|---|---|---|---|---|---|---|---|
| 2 | 12555.97 | 11803.10 | 12610.26 | < .001 | < .001 | < .001 | .808 | none |
| 3 | 11945.07 | 12021.08 | 11976.61 | < .001 | < .001 | < .001 | .866 | 0 |
| 4 | 11705.37 | 11803.10 | 11745.92 | < .001 | < .001 | < .001 | .780 | 0 |
| 5 | 11590.61 | 11710.05 | 11640.16 | < .001 | < .001 | < .001 | .794 | 1 |
| 6 | 11553.95 | 11695.12 | 11612.52 | .054 | .059 | < .001 | .721 | 1 |
| 7 | 11523.35 | 11686.23 | 11590.93 | .755 | .761 | < .001 | .741 | 2 |
Note. AIC = Akaike Information Criteria; BIC = Bayesian Information Criteria; LRT = Vuong-Lo-Mendell-Rubin Likelihood-Ratio Test; BLRT = Bootstrap Likelihood Ratio Test; d = effect size. Fit criteria indicating the best model are printed in bold.
The models with five, six and seven latent profiles exhibit lower AIC and BIC values, entropy values of .7, and, for the five-profile model, p < .05 for the LRT. However, this model is rejected because it displays a cluster that includes less than 1% of the sample. Similarly, the six and seven-profile models are also rejected for two reasons: the p-value of the LRT is over .05 and they contain a cluster with less than 1% of the sample. On the other hand, it can be observed that, among the remaining models, the four-profile model provides the best fit to the data because it exhibits the lowest AIC and BIC values compared to the two and three-profile models, since these are preferent criteria even though this model did not exhibit the highest entropy index (.78), it also exhibits a statistically significant p-value (p < .05) for both the LRT and the BLRT, indicating a superior fit compared to the alternative models. Furthermore, all the groups in the four-profile model are representative of the sample. Hence, this model of latent profiles is chosen for conducting the subsequent data analysis. The selection of the four-profile solution is also based on its greater theoretical interpretability, consistent with prior literature on social anxiety (Sanmartín et al., 2020; Yu et al., 2020).
In terms of interpretability and psychological significance, the chosen solution classified social anxiety into four different profiles. The first profile, named Mild SA, consisted of 490 adolescents (29.1%) with low (clinically insignificant) scores across all three dimensions of social anxiety, that is, despite experiencing some nervousness in social contexts, these adolescents are relatively functional. The second profile, named Moderate SA, included 629 students (37.3%) with moderate levels of social anxiety, which could interfere with their life with symptoms such as embarrassment, avoidance of social situations and public speaking difficulties. The third profile, known as Severe SA, had 498 individuals (29.6%) who reported high scores in all three dimensions of the SAS-A with symptoms such as isolation, panic attacks, and physical symptoms such as heartbeat or nausea. Finally, the fourth profile, labeled Extreme SA, included 68 participants (4.0%) who had very high scores in social anxiety that could met the criteria for social anxiety disorder (SAD) which can indicate a significant impairment in functioning. For the 4-latent profile model, Figure 1 presents the standardized means of the SAS-A factors, representing the three dimensions of social anxiety (FNE, SAD-N, and SAD-G) for each student profile.

According to the chi-squared test (χ2 = 3.53, p = .317), the distribution of males and females in each latent profile was similar, so no significant gender differences were found in the proportions of each profile (Table 4).
Inter-group differences in interpersonal difficultiesThe purpose of the MANOVA was to examine the average scores of the interpersonal difficulties among the different social anxiety profiles. The results of the MANOVA indicated statistically significant differences between the latent social anxiety profiles across all dimensions of the QIDA (Wilks’ lambda = .85, F(15.1861) = 18.62, p < .001, np2 = .05). If the F -value is large, and its associated p < .001, at least one of the dependent variables differs significantly among the groups. The variables assertiveness (AS), heterosexual relationships (HR), public speaking (PS), family relationships (FR) and close friendships (CF) showed significant differences among the four social anxiety profiles (see Table 5). Among these variables, the mild SA profile (Cluster 1) had the lowest mean scores in all dimensions of the QIDA, whereas the extreme SA profile obtains the highest mean scores in all dimensions of the QIDA.
Means and standard deviations of each latent profile and statistical significance
| Mild SA profile | Moderate SA profile | Severe SA profile | Extreme SA profile | Statistical Significance | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Dimensions | M | SD | M | SD | M | SD | M | SD | F(3,1581) | p |
| AS | 32.95 | 8.32 | 36.98 | 8.19 | 40.61 | 9.53 | 41.92 | 12.51 | 68.68 | < .001 |
| HR | 16.22 | 6.77 | 19.59 | 6.57 | 21.19 | 7.17 | 22.54 | 8.25 | 50.53 | < .001 |
| PS | 10.96 | 3.43 | 12.35 | 3.51 | 13.30 | 3.77 | 14.00 | 5.05 | 39.35 | < .001 |
| FR | 6.63 | 2.59 | 7.34 | 2.71 | 8.06 | 2.86 | 8.07 | 3.02 | 23.93 | < .001 |
| CF | 6.02 | 2.06 | 6.69 | 2.26 | 7.41 | 2.57 | 7.61 | 2.76 | 32.61 | < .001 |
Note. SA = social anxiety; AS = assertiveness; HR = heterosexual relationships; PS = public speaking; FR = family relationships; CF = close friendships.
Differences in QIDA factor scores among SAS-A clusters are presented in Table 6. Regarding the assertiveness variable, high effect sizes are observed between cluster 1 and 4 (d = 1.01), and cluster 1 and 3 (d = 0.85). The effect size is moderate between cluster 2 and 4 (d = 0.57) and decreases between clusters 1 and 2 (d = 0.49) and cluster 2 and 3 (d = 0.42). For the heterosexual relationships variable, a high effect size can be found between cluster 1 and 4 (d = 0.91). Moderate effect sizes can be observed between cluster 1 and 3 (d = 0.71) and cluster 1 and 2 (d = 0.51) while the effect size decreases between clusters 2 and 4 (d = 0.44) and cluster 2 and 3 (d = 0.23). Concerning the public speaking variable, the effect size is high between cluster 1 and 4 (d = 0.83). Moderate effect sizes can be found between cluster 1 and 3 (d = 0.65) and the effect size decreases between clusters 2 and 4 (d = 0.45), cluster 1 and 2 (d = 0.40) and cluster 2 and 3 (d = 0.26).
Differences in QIDA factor scores among SAS-A clusters
| Dimensions | 1-2 mild SA vs moderate SA | 1-3 mild SA vs severe SA | 1-4 mild SA vs extreme SA | 2-3 moderate SA vs severe SA | 2-4 moderate SA vs extreme SA | 3-4 severe SA vs extreme SA | |
|---|---|---|---|---|---|---|---|
| AS | p | < .001 | < .001 | < .001 | < .001 | < .001 | n. s. |
| d | 0.49 | 0.85 | 1.01 | 0.42 | 0.57 | - | |
| HR | p | < .001 | < .001 | < .001 | .001 | .005 | n. s. |
| d | 0.51 | 0.71 | 0.91 | 0.23 | 0.44 | - | |
| PS | p | < .001 | < .001 | < .001 | < .001 | .002 | n. s. |
| d | 0.40 | 0.65 | 0.83 | 0.26 | 0.45 | - | |
| FR | p | < .001 | < .001 | < .001 | < .001 | n. s. | n. s. |
| d | 0.27 | 0.52 | 0.54 | 0.26 | - | - | |
| CF | p | < .001 | < .001 | < .001 | < .001 | .012 | n. s. |
| d | 0.31 | 0.59 | 0.74 | 0.30 | 0.40 | - |
Note. SA = social anxiety, AS = assertiveness, HR = heterosexual relationships, PS = public speaking, FR = family relationships, CF = close friendships.
Regarding the family relationships variable, the effect size is moderate between cluster 1 and 4 (d = 0.54) and cluster 1 and 3 (d = 0.52). The effect size decreases between clusters 1 and 2 (d = 0.27) and cluster 2 and 3 (d = 0.26). There is no statistically significant difference between cluster 2 and 4 for this variable. For the close friendships variable, the effect sizes are moderate between cluster 1 and 4 (d = 0.74) and cluster 1 and 3 (d = 0.59). The effect size decreases between clusters 2 and 4 (d = 0.40), cluster 1 and 2 (d = 0.31) and cluster 2 and 3 (d = 0.30). Finally, it should be highlighted that there are no statistically significant differences between the severe social anxiety (cluster 3) and extreme SA (cluster 4) groups in any of the QIDA variables.
DiscussionThe general objective of this study was to examine the existence of statistically significant differences between potential adolescents’ social anxiety profiles on the interpersonal difficulties dimensions, that is, assertiveness, heterosexual relationships, public speaking, family relationships and close friendships, in a representative sample of Spanish adolescents enrolled in Secondary Education. For this purpose, latent profile analysis was used to identify and classify homogeneous subgroups of participants with different patterns of social anxiety. This methodology aimed to facilitate early identification, detection, and intervention measures for different subgroups, aiming to prevent the potential negative impact of social anxiety on interpersonal difficulties at various levels, including personal, school, family, romantic relationships and friendships. In this study, four latent profiles were identified based on social anxiety assessed using the SAS-A. The identified profiles represented different levels of social anxiety.
The findings support the first hypothesis of the study, since four profiles were identified. These results coincide with the number of social anxiety groups found in previous literature (Camacho et al., 2022; Dell’Osso et al., 2014; Fernández-Sogorb et al., 2022; Furmark et al., 2000; Piqueras et al., 2008; Tillfors et al., 2004). Thus, participants with low, moderate, high, and excessive (SAD) levels of social anxiety are grouped into the mild SA, moderate SA, severe SA, and extreme SA groups, respectively. Considering the adequacy of the LPA to identify homogeneous latent profiles it is basic to continue researching on the social anxiety profiles, carrying out LPA with Spanish adolescents to corroborate the four groups.
Regarding the interpersonal difficulties dimensions, the extreme SA group is the one with the highest problems in assertiveness, heterosexual relationships and public speaking, and the only subgroup that presents difficulties with close friendships. The severe SA profile exhibits high difficulties in assertiveness and some difficulties with heterosexual relationships and public speaking as well. Since no group exhibits high difficulties in family relationships, on-site interventions should focus on assertiveness and social interactions.
Regarding the differences between the adolescent social anxiety groups on interpersonal difficulties, the findings of the present investigation are in line with those of Sanmartín et al. (2020) who conducted a study with Ecuadorian adolescents and discovered that students classified as having a self-fulfilling profile (less interpersonal difficulties) had the lowest scores for social anxiety, whereas those with a self-destructive profile (more interpersonal difficulties) showed the highest scores of social anxiety. The study by Tonge et al. (2020) reveals that interpersonal difficulties in individuals with generalized social anxiety disorder (SAD) differ depending on the type of relationships they are involved in. Assessing and addressing these difficulties within specific contexts, such as family and school, is essential to understand the impact of roles and expectations on behavioral problems. No statistically significant differences were identified in Family relationships in any latent profile. Targeted interventions to improve interpersonal functioning are vital for a comprehensive understanding of social anxiety. Factors like timing, location, and individual differences contribute to our understanding of the impact of social anxiety on interpersonal difficulties.
In addition to the contributions of this study, caution should be exercised when interpreting the results due to the limitations of the study that should be considered in future research. Firstly, the identification of adolescent social anxiety profiles was based on a community sample in Secondary Education, and it remains unclear whether similar profiles exist in other educational levels. Secondly, a limitation inherent to the QIDA is the measurement and evaluation of the adolescents' difficulties with peers of the opposite sex. To address this limitation, the development and psychometric validation of the QIDA should be reformulated and undoubtedly include the difficulties adolescents experience when interacting with someone they are emotionally and/or sexually attracted to, regardless of their sexual orientation. Thirdly, to determine the generalizability of findings, future studies should include adolescent populations from different geographic areas within Spain and samples from various educational levels to investigate the replicability of the four-profile model. Previous research, which focused on similarities and differences in social anxiety levels among university students of the same gender across 17 Spanish Autonomous Community regions, revealed minimal disparities in social anxiety within this cohort (e.g., Caballo, Salazar, Arias et al., 2010).
Furthermore, it is essential to examine social anxiety profiles in adolescence across different countries to explore potential cultural variations, since generalizing the results to other countries is not possible due to known cross-cultural differences in social anxiety since social norms and cultural values, such as individualism-collectivism, can influence the significance, intensity, and symptoms of social anxiety (Torregrosa et al., 2022; Zhou et al., 2008). Previous studies have already examined the multidimensional nature and multicultural validity of the Social Anxiety Questionnaire for Adults (SAQ-A) through studies involving adults from 18 to 20 different countries (Caballo et al., 2012, 2014, 2015). Understanding social anxiety in adolescents from different cultural contexts can provide valuable information regarding the cultural specificity of these profiles. Moreover, due to the potential sources of bias in self-reported data, such as social desirability or response bias, it is advisable to be cautious when interpreting results obtained from the use of self-report questionnaires.
In addition, by using the clinical cut-off points of the SAS-A in the Spanish adolescent population (Olivares et al., 2002) to establish subclinical social anxiety levels, it remains unknown how many adolescents had a clinically significant social anxiety. In future investigations it might be interesting to conduct the latent profile analysis with all factors of social anxiety and interpersonal difficulties together. Addressing these limitations in future research would contribute to our understanding of social anxiety profiles in adolescence and provide more robust evidence regarding the associations between social anxiety and interpersonal difficulties in adolescence.
This research has significant implications for educational practice. It is essential to implement early preventive interventions and identify adolescents who are at risk for social anxiety. Improving peer relationships and addressing social anxiety can help prevent psychological issues in adolescents (Chiu et al., 2021). One of the most effective cognitive-behavioral intervention techniques that significantly improves the efficacy of social skills training for adolescents without significant social problems is the modeling of prosocial behaviors performed by socially skilled peers (Inglés, Martínez-Monteagudo et al., 2008). In addition, cooperative learning interventions are beneficial for improving social skills. Working together in groups creates opportunities for peers to interact, collaborate, and learn from each other (Fernández-Río et al., 2022). Teamwork and mutual support create a sense of community, a positive social environment that benefits adolescents both academically and socially.
Two potential social anxiety risk profiles have been identified within the Spanish adolescent population. The severe SA profile, comprising 29.6% of the participants, is characterized by high levels of social anxiety and interpersonal difficulties. Conversely, the extreme SA profile includes 4.0% of the participants and comprises excessive levels of social anxiety. Considering these findings, it is indispensable for teachers to critically examine their educational practices and establish supportive relationships with students with social anxiety, taking into consideration their interpersonal difficulties (e.g., providing support to newcomers through buddy systems, planning school-based social activities or teaching how to improve peer relationships).
The development of adolescents' social behaviors is the goal of a number of social skills programs addressed to teachers (Chen, 2006). Implementing intervention programs for adolescents with high social anxiety (e.g., La Greca et al., 2016) can promote positive relationships among students. Chen (2006) concluded that teaching social skills directly is an effective intervention which helps adolescents develop positive socially accepted behaviors and build good relationships; it improves academic success and contributes to better relationships with peers, family, and other adults. A pilot study investigating the effects of the Interpersonal Skills Training Program for Adolescents (ISTA, PEHIA in Spanish) (Inglés, 2003) on a Spanish student sample demonstrated promising results in reducing anxiety, particularly in assertiveness, interpersonal relationships, and public speaking skills (Serrano-Pintado et al., 2022). The Multidimensional Intervention for Social Anxiety program (MISA) integrates the most effective intervention strategies available for both general social anxiety and social anxiety disorder while not only improving individuals' social lives but enhancing their overall quality of life (Caballo et al., 2019, 2021; Salazar et al., 2022).
The Skills for Academic and Social Success program (SASS) is a school-based intervention using cognitive-behavioral techniques for adolescents diagnosed with social anxiety disorder (Fisher et al., 2004). This program emphasizes social skills and in-vivo exposure. Meta-analytic studies and independent researchers have demonstrated the effectiveness of the Intervention for Adolescents with Social Phobia (IAFS; Olivares & García-López, 1998) program (Gil-Bernal & Hernández-Guzmán, 2009; Olivares, 2011; Olivares & García-López, 2001).
To enhance the effectiveness of social anxiety interventions and minimize negative effects on peer relationships, the implementation of a more individualized approach is recommended (Camacho et al., 2022). This approach involves distinguishing between different social anxiety profiles and considering their unique dynamics. By recognizing and addressing the specific needs and challenges associated with each profile, interventions can be tailored more precisely to individuals' differences. This personalized approach has the potential to improve intervention outcomes, promote better relationships with peers and contribute to the adolescent’s overall well-being.
Despite the limitations of the study, it has some theoretical contributions. The observed correlation between social anxiety and interpersonal difficulties could be explained by the fact that three of the variables, assertiveness, heterosexual relationships and public speaking, are considered inherent dimensions to the construct of social anxiety in other studies (e.g., Caballo, Salazar, Irurtia et al., 2010; Caballo et al., 2012, 2015). The findings of this study support the existence of diverse profiles in social anxiety related to interpersonal difficulties in a sample of Spanish adolescents. Although beneficial for all adolescents, these results are particularly essential for those with high or excessive levels of social anxiety and interpersonal difficulties, which may refuse school to avoid social situations and interpersonal difficulties (e.g., oral exams, presentations, collaborative work, socializing with peers, etc.). The role of parents and friends have a significant impact on the academic and career prospects of adolescents (e.g., Martínez-González et al., 2010). To prevent interpersonal difficulties in adolescents which might interfere in their teaching-learning process, it is recommended to implement on-site interventions for social anxiety to help adolescents perceive secondary school as a safe and supportive environment.
FinancingThis research work has not received any type of specific financial support from public, private, or non-profit institutions.
Conflict of interestsThe authors declare no conflicts of interest.
The authors express their gratitude to the teachers who participated in data collection and to the students who willingly took part in this study.
