




The study aimed to compare the effectiveness of computer-based teaching and face-to-face teaching strategies in terms of knowledge of clinically related courses among newly hired oncology nurses.
Material and methodsA 2-group pre- and post-test design was performed. The study included 128 participants. The participants were randomly assigned into the study groups (control and experimental groups). Both groups attended a course on the SBAR technique, with one group using face-to-face teaching and the other using computer-based learning.
ResultsThe study included 128 participants. Of them, 36.7% are male (n=47). The total mean age was 22.19 (SD=0.94). The total mean of the pre-test was 3.81/7 while the post-test was 5.82/7 for the experimental group. The total mean of the pre-test was 3.78/7, while the post-test was 5.51/7 for the control group. The paired t-test results showed that the differences between the pre- and post-test mean for each group were significant. The results showed no significant difference in the pre-test means between the experimental and control groups (p-value=.913). The difference in post-test mean between the experimental and control groups was significant (p-value=.04).
ConclusionOur findings suggest that both computer-based and face-to-face teaching strategies effectively increased knowledge levels among newly hired nurses. Importantly, the computer-based teaching approach demonstrated a statistically significant superiority in knowledge retention compared to face-to-face teaching.
El estudio tuvo como objetivo comparar la efectividad de las estrategias de enseñanza basadas en ordenador y cara a cara en términos de conocimiento de cursos clínicamente relacionados entre enfermeros de oncología recién contratados.
Materiales y métodosSe realizó un diseño de pre y postprueba de dos grupos. El estudio incluyó 128 participantes. Los participantes fueron asignados al azar a los grupos de estudio (grupos de control y experimentales). Ambos grupos asistieron a un curso sobre la técnica SBAR, siendo un grupo instruido mediante enseñanza presencial y el otro a través de aprendizaje basado en ordenador.
ResultadosEl estudio incluyó 128 participantes. De ellos, el 36.7% eran hombres (n = 47). La edad media total fue de 22.19 (SD = 0.94). La media total de la preprueba fue de 3.81/7, mientras que la de la posprueba fue de 5.82/7 para el grupo experimental. La media total de la preprueba fue de 3.78/7, mientras que la de la posprueba fue de 5.51/7 para el grupo de control. Los resultados de la prueba t pareada mostraron que las diferencias entre la media de la preprueba y la posprueba para cada grupo fueron significativas. Los resultados mostraron que no hubo una diferencia significativa en las medias de la preprueba entre los grupos experimental y de control (valor de p = 0.913). La diferencia en la media de la posprueba entre los grupos experimental y de control fue significativa (valor de p = 0.04).
ConclusiónLa enseñanza basada en ordenador también puede considerarse una estrategia efectiva de enseñanza de habilidades de enfermería clínica. Nuestros hallazgos sugieren que tanto las estrategias de enseñanza basadas en ordenador como las presenciales aumentaron de manera efectiva los niveles de conocimiento entre las enfermeras recién contratadas. Importante destacar que el enfoque de enseñanza basado en ordenador mostró una superioridad estadísticamente significativa en la retención del conocimiento en comparación con la enseñanza presencial.
Computer-based teaching sessions have benefits over face-to-face teaching sessions1. They are more adaptable to students' work and learning schedules and have the option to pause or return to certain parts of the session. They allow for more learner-led interaction; hyperlinks and supplementary materials can be given to the learner immediately. They address the cost and logistical challenges of specialist lecturers teaching large groups of students in various places, as well as the issue of standardizing the quality of teaching materials across an area. The use of computer-based teaching sessions in college classrooms is continuing to grow. The importance of using technologies such as computer-based learning in different disciplines is discussed in the literature. Researchers have measured the effectiveness of computer-based learning in many fields including the nursing field.2
Within the health professions such as nursing professions, a large portion of the curriculum allows students to learn clinical skills firsthand3. Traditionally, these skills have been taught in a face-to-face setting, with the instructor demonstrating clinical skills and the students practicing them2,4. In addition to the acquisition of clinical skills, nursing education recognizes the paramount importance of soft skills, encompassing interpersonal communication, teamwork, and critical thinking. These skills, often referred to as ‘soft’ due to their non-technical nature, are integral to effective nursing practice. Interpersonal communication skills enable nurses to establish meaningful connections with patients, while teamwork skills facilitate collaboration within multidisciplinary healthcare teams. Critical thinking, another essential soft skill, empowers nurses to navigate complex clinical situations and make informed decisions. While not directly involving physical patient care, these soft skills significantly contribute to the overall competence of nurses and are essential components of our study evaluating the comparative effectiveness of computer-based versus face-to-face teaching for newly hired oncology nurses.
The e-Learning system was introduced for the nurses' staff training after a significant development of technology and e-health in terms of high Internet speed, accessibility, and conductivity2,5. This system has moved nurse education in the clinical setting from the face-to-face lecture-based teaching format to computer-based teaching sessions.
Studies of nurses' skills and attitude change as result of computer-based teaching sessions showed that nurses who received computer-based learning had better knowledge than nurses who received the face-to-face learning-based teaching1,6. The other studies showed that there are no differences between 2 modalities7. Some studies indicated that the face-to-face teaching-based learning is more suitable when the study content focuses more on clinical skills8.
The majority of these research were unregulated, small observational studies performed solely for theoretical material. It is perhaps a foregone conclusion that the bulk of nursing education would be done on computers. But, at the moment, there is little high-quality evidence in the form of randomized controlled trials to back this up. As a result, it is critical to develop this evidence base for nursing education and learning in the clinical environment2,9,10. The use of computer-based teaching may help to improve nursing education. The effective learning of newly hired nurses is usually influenced by external factors such as instruction, simulation, and exams. It may be possible to draw the nurses away from such shallow learning styles by using the benefits of computer-based learning to build immersive packages that facilitate deeper learning2,11.
Randomized controlled trials may provide strong proof of educational effectiveness1. 55 new doctors were randomly assigned to either computer-based sessions or an analogous lecture in EBM and systematic reviews in a randomized controlled trial. A validated questionnaire was used to evaluate skills (primary outcome) and attitudes (secondary outcome) before and after the intervention (secondary outcome). At the baseline, both groups were close. The computer-based group gained the same amount of information as the lecture-based group (gain in score: 2.1 [SD=2.0] versus 1.9 [SD=2.4]; ANCOVA P=.078). In both classes, the gains in attitude were identical1.
In education, randomized trials may suffer from difficulties with contamination between study arms, inability to blind study participants and teachers from educational intervention(s), standardizing educational interventions, and measuring outcomes such as knowledge retention and compliance with the standards due to a lack of valid and reliable assessment tools1,4,8.
We conducted a randomized controlled trial comparing 2 teaching methods that were designed to avoid the issues listed above. We hypothesized that both teaching methods would be equally successful in improving the learning of newly employed nurses.
MethodsDesignA 2-group pre- and post-test design was performed to evaluate the effectiveness of teaching using self-administered questionnaires before and after implementing the teaching techniques. These designs aid in explaining and determining the interventions' effects12. This design was used to address some of the shortcomings of previous studies that used descriptive pre- and post-test designs, or used pre- and post-test in one group only.
SettingThe study was carried out at the King Hussein Cancer Center (KHCC), a nongovernmental, non-profit, specialized center in Amman, Jordan. Every year, this hospital treats over 3500 new cancer patients locally, nationally, and globally. This hospital had developed services that focused on all aspects of cancer care, from prevention and early detection to diagnosis and treatment, as well as palliative care. There are more than 1000 nurses working at the hospital.
SampleSince previous research did not include a straightforward power analysis, it is recommended that traditional effect sizes to be used (Cohen, 1988). As a result, the sample size was calculated using power analysis with a medium effect size of 0.5, a significance alpha of 0.05 (two-tailed), and a power of 0.8, yielding a sample size of 128. Accordingly, 64 nurses were selected using a random sampling technique and randomly assigned to each group. Newly trained nurses with no prior experience and who were newly employed as clinical nurses in inpatient units at King Hussein Cancer Center were considered eligible.
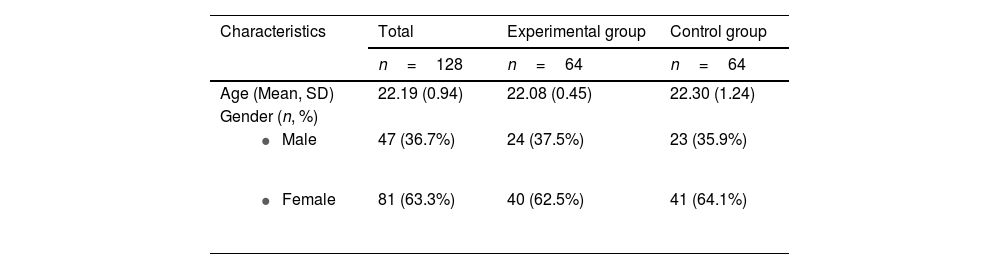
DemographicsThe study included 128 participants. Of them, 36.7% are male (n=47). The total mean age was 22.19 (SD=0.94). The participants were randomly assigned into the 2 study groups (control and experimental groups). In the experimental group, 37.5% are male (n=24) and the total mean age was 22.08 (SD=0.45) while around 35.9% are male (n=23) and the total mean age was 22.30 (SD=1.24). All participants held a bachelor's degree in nursing (Table 1).
InterventionThe first group attended a specific course utilizing a face-to-face learning-based teaching that was considered the existing situation. The second group attended the same course but using computer-based teaching (recorded course). The course was about the SBAR (Situation-Background-Assessment-Recommendation) technique that is used as a framework for healthcare team members to communicate in a structured way about a patient's condition. This course was selected due to its importance, knowing that effective communication is an international patient safety goal as indicated by The Joint Commission13. The course content was similar for both groups. The content was mainly developed according to Institute for Healthcare Improvement (IHI). The education material was reviewed by 3 nurse quality supervisors.
Rigorous measures were taken to minimize potential biases and confounding variables regarding internal validity. Random assignment was employed to ensure comparability between the experimental and control groups, and careful selection of the control group further contributed to the internal validity of our study.
The effectiveness of the intervention was determined by testing the knowledge level before and after the intervention for each group. The multiple choice test was prepared according to the study material. The test was reviewed by the nursing professional development team. The age, educational level, and gender of participants were added to the demographic section of the test.
ProcedureThe pre-test was conducted for both groups in order to measure the baseline level of knowledge in the chosen content. A demographic sheet was initially distributed, then an educational session using the traditional lecturing (SBAR technique) was provided for the first group and a computer-based learning technique was provided in the computer lab for the second group. The presentations were saved in the computer lab in KHCC for the experimental group. Then, a post-test survey was immediately conducted for both groups to measure knowledge retention. In this study, we specifically focus on giving more detail about the kind of interventions that were faced by the experimental (computer-based teaching) and control (face-to-face teaching) groups. In the experimental group, however, a specially designed course itself which consisted of computer-related learning with special attention regarding the SBAR approach was carried out. The recording of all the course content was supposed to be available in the computer lab where students could tend to move through the material according to their convenience. The content was reviewed by 3 experts in the field to ensure its instructional validity according to the needs set by IHI. The other group, on the other hand, went through a similar course that incorporated the old orthodox one-on-one teachings methods with an equal emphasis of the SBAR technique. Clearly, both groups had the same materials meaning that there were intentions to have uniformity in the teaching material.
Data analysis methodData were analyzed using a Statistical Package of Social Science version number 22. Descriptive statistics were used based on the level of measurement to describe the study variables. Also, a t-test was used to assess the differences between the 2 groups. Independent and paired t-tests were used to assess the differences between age groups. Moreover, Pearson's correlation (r) was used to determine the relationship between computer-based teaching, traditional teaching, and knowledge outcome.
Ethical considerationsPrior to data collection, ethical approval for conducting the study was obtained from the Ethics Committee of the Institutional Review Board of the hospital in which the study was to be conducted. Newly hired nurses who participated in the study signed informed consent forms, and their confidentiality was assured during all phases of the study. All nurses were informed that they can withdraw from the study at any time and this was not affect their employment. Nurses were assured that participation is voluntary, their personal information and the (pre and post) tests results were kept in a safe place, the data and results were originated from the study were used for research purposes, and the results did not affect their employment status.
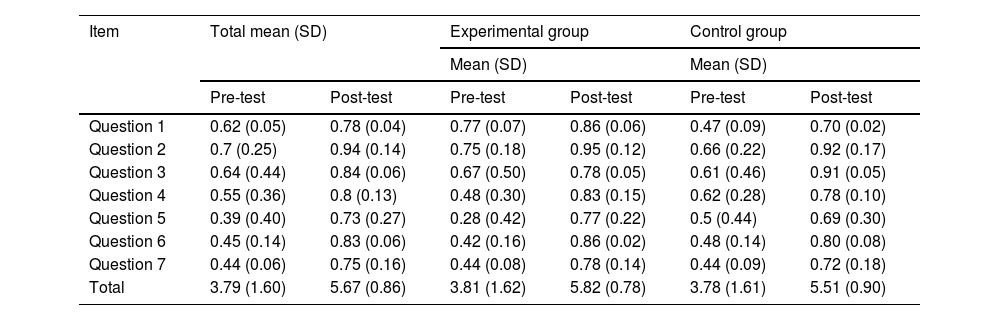
ResultsMean values of study groupsTable 2 presented the mean values for the mean of pre- and post-tests. The results showed that the total mean of the pre-test was 3.79/7 while the post-test was 5.67/7 for the total sample. The total mean of the pre-test was 3.81/7 while the post-test was 5.82/7 for the experimental group. The total mean of the pre-test was 3.78/7, while the post-test was 5.51/7 for the control group. Moreover, the numbers of attitudinal gains achieved are close to each other (see Fig. 1).
Mean values.
| Item | Total mean (SD) | Experimental group | Control group | |||
|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | |||||
| Pre-test | Post-test | Pre-test | Post-test | Pre-test | Post-test | |
| Question 1 | 0.62 (0.05) | 0.78 (0.04) | 0.77 (0.07) | 0.86 (0.06) | 0.47 (0.09) | 0.70 (0.02) |
| Question 2 | 0.7 (0.25) | 0.94 (0.14) | 0.75 (0.18) | 0.95 (0.12) | 0.66 (0.22) | 0.92 (0.17) |
| Question 3 | 0.64 (0.44) | 0.84 (0.06) | 0.67 (0.50) | 0.78 (0.05) | 0.61 (0.46) | 0.91 (0.05) |
| Question 4 | 0.55 (0.36) | 0.8 (0.13) | 0.48 (0.30) | 0.83 (0.15) | 0.62 (0.28) | 0.78 (0.10) |
| Question 5 | 0.39 (0.40) | 0.73 (0.27) | 0.28 (0.42) | 0.77 (0.22) | 0.5 (0.44) | 0.69 (0.30) |
| Question 6 | 0.45 (0.14) | 0.83 (0.06) | 0.42 (0.16) | 0.86 (0.02) | 0.48 (0.14) | 0.80 (0.08) |
| Question 7 | 0.44 (0.06) | 0.75 (0.16) | 0.44 (0.08) | 0.78 (0.14) | 0.44 (0.09) | 0.72 (0.18) |
| Total | 3.79 (1.60) | 5.67 (0.86) | 3.81 (1.62) | 5.82 (0.78) | 3.78 (1.61) | 5.51 (0.90) |

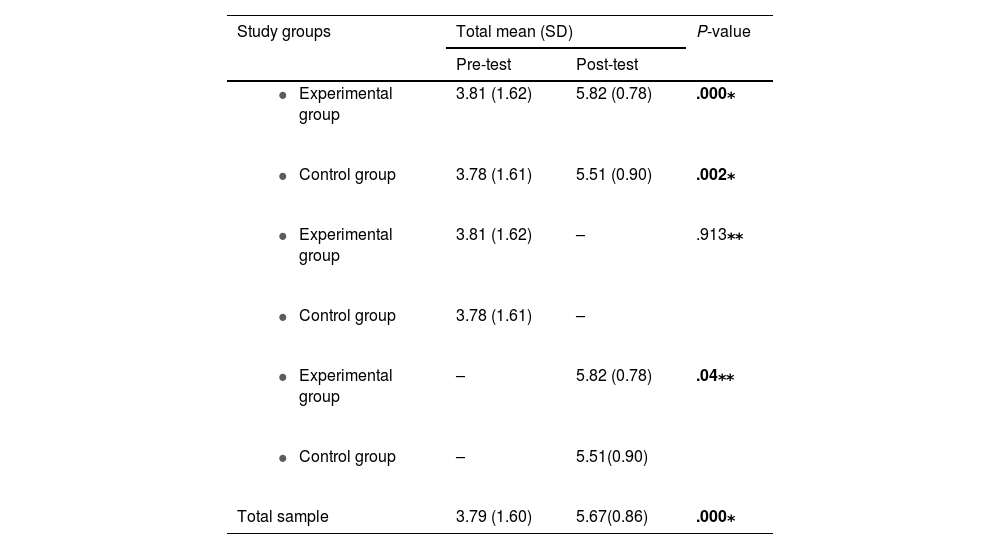
Table 3 presented the mean difference between study groups. The results showed significant differences between the pre- and post-test means for the total sample (P-value=.000). Moreover, the paired t-test results showed that the differences between the pre- and post-test mean for each group were significant. However, the P-value between the pre- and post-test means in the experimental group (P-value=.000) was lower than the P-value between the means in the control group (P-value=.002). The results showed no significant difference in the pre-test means between the experimental and control groups (P-value=.913). The difference in post-test mean between experimental and control groups was significant (P-value=.04).
Mean differences between study groups.
| Study groups | Total mean (SD) | P-value | |
|---|---|---|---|
| Pre-test | Post-test | ||
| 3.81 (1.62) | 5.82 (0.78) | .000⁎ |
| 3.78 (1.61) | 5.51 (0.90) | .002⁎ |
| 3.81 (1.62) | – | .913⁎⁎ |
| 3.78 (1.61) | – | |
| – | 5.82 (0.78) | .04⁎⁎ |
| – | 5.51(0.90) | |
| Total sample | 3.79 (1.60) | 5.67(0.86) | .000⁎ |
This study found that when teaching a clinically oriented course like SBAR in our setting, there was a gap between computer-based sessions and lectures in terms of experience in an oncology setting. We suggested that computer-based instruction could be preferable for a focused clinical course, and we confirmed that computer-assisted instruction is not inferior to lectures since attitudinal gains were similar to each other as a secondary outcome.
Our research is the first of its kind in the field of nursing education. We were able to report in accordance with the CONSORT guidelines. Randomization was concealed, all treatments were administered by the same teacher, no interventions were contaminated, the evaluation was checked and blinded, and the capacity was adequate to show non-inferiority. The sample size is appropriate to make the generalization to the same setting and population and to address our null hypothesis. The trial forms the groundwork for the creation, adaptation, and evaluation of new computer-based learning strategies for use in continuing education for nurses. This highlights the importance of computer-assisted instruction, which can be made accessible whenever students want. The results showed no significant difference in the pre-test means between the experimental and control groups (P-value=.913). The result indicate the level of similarity between the two groups before conducting the intervention.
The paired t-test results showed that the differences between the pre- and post-test mean for each group were significant, which means that both strategies are effective in increasing the knowledge levels among nurses. However, the P-value between the pre- and post-test means in the experimental group was lower than the P-value between the means in the control group which may be explained by the significant difference in post-test mean between the experimental and control groups was significant. These results indicate that the level of knowledge among nurses who attend the computer-based course was higher than the level of knowledge among nurses who attend the face-to-face course. In other words, the results showed that the computer-based teaching was more effective than face-to-face teaching. Our research indicates a significant improvement in knowledge retention among newly employed oncology nurses who received computer-based training. However, it is essential to approach the comparison with face-to-face teaching comprehensively. The statistics suggest a notable difference in knowledge retention between the computer-based and face-to-face teaching groups, indicating a possible superiority of the former over the other 2 types of education.
While our study primarily focused on evaluating the impact of teaching methodologies, specifically the SBAR technique, on soft skills such as interpersonal communication, teamwork, and critical thinking, we acknowledge the broader spectrum of nursing skills that encompass practical procedures in the clinical setting. Practical procedures are fundamental to nursing education and practice, and their exclusion from our study's scope is a notable limitation. It is crucial to recognize that the effectiveness of teaching strategies extends beyond soft skills to include the development of hands-on clinical competencies. Future research could explore the differential impact of computer-based versus face-to-face teaching on both soft skills and practical procedures to provide a more comprehensive understanding of nursing education outcomes.
Nevertheless, it is crucial to recognize that several circumstances may impact educational achievements, and the noted difference does not indicate a definitive superiority of one learning method over the other in every situation. The study we conducted at the King Hussein Cancer Centre adds to the increasing evidence that supports the effectiveness of computer-based teaching. However, we acknowledge the necessity of further investigation in various clinical settings to determine the applicability of these findings.
The following are the characteristics of this research that demonstrated the efficacy of computer-based learning: The face-to-face lecture and computer-based learning were given by the same speaker. We attempted to take special care to develop a high-quality e-content that was checked and validated by experts in that field before interventions, even though the students in the computer-based learning community had no time limit for reviewing the lesson. We planned the RCT in such a way that it avoided the difficulties of educational RCTs to the greatest extent possible.
Our results have ramifications for how the new nurses are trained. Computer-based learning has the ability to fulfill training needs, and it is also being used in continuing professional education by other professionals. Our research indicates that, at least for the teaching of SBAR, computer-based instruction is a feasible alternative to lectures. It would be available at other times for those who did not attend sessions, while lectures could not be easily replicated. According to the findings of other research, study participants were less satisfied with the computer-based strategy than with the other methods, such as lecture-based teaching2.
We want to clarify that our study does not seek to universally assert the superiority of computer-based education over face-to-face education. We acknowledge that educational methodologies can vary across disciplines and contexts. The statement about skill and attitude change as a result of computer-based education sessions merely reflects an observation from existing literature, not a claim made by our study. Our research is specific to the field of oncology nursing and is intended to contribute valuable insights into the effectiveness of computer-based teaching compared to face-to-face teaching within this particular domain. We appreciate the importance of recognizing the diversity of educational settings, and our study aims to provide evidence-based findings in the context of clinically related courses for newly hired oncology nurses.
This will be a huge benefit for nurses who are constantly pressed for time. Computer-based sessions also make it easier to standardize teaching across institutions and overcome the challenge of teaching a broad group of students who are spread across many locations. To promote deeper learning, computer-based learning can be made interactive through the integration of engaging features designed to actively involve learners in the educational process. One effective strategy is the incorporation of realistic simulations, providing learners with immersive scenarios that mirror the complexities of the clinical setting. Simulations offer a safe space for applying theoretical knowledge to practical situations, fostering critical thinking and decision-making skills. Additionally, the inclusion of case studies within computer-based modules enables learners to analyze real-life healthcare scenarios, encouraging problem-solving and a deeper understanding of the subject matter. Interactive exercises, including quizzes, discussions, and collaborative activities, further enhance engagement, facilitating active participation and knowledge retention. The adaptability of computer-based learning allows learners to progress at their own pace, revisit challenging topics, and receive immediate feedback, reinforcing the learning process. In summary, the interactive elements in computer-based learning contribute to a dynamic and multifaceted educational experience that goes beyond traditional methods, cultivating both theoretical understanding and essential practical skills for effective nursing practice.
The inclusion of links to information found on the Internet or in other files will help to improve the learning experience1,14. For 2 reasons, we did not discuss participants' long-term knowledge maintenance: first, there could be post-intervention cross-contamination, and second, the participants' long-term knowledge could not be definitively linked to our intervention due to their further analysis of the subject. This limitation has been discussed in studies that have assessed long-term information maintenance.
Although this research showed significant enhancements in information retention among recently employed oncology nurses who were exposed to computer-based instruction, it is crucial to evaluate the study's validity carefully. To ensure internal validity, we used rigorous methods such as random assignment and meticulous selection of control groups in order to minimize possible biases and improve the dependability of our findings.
By recognizing particular limits, such as limitations in sample size and the unique features of the research population, we provide further context to our results. In order to assess the external validity of our research, we have conducted a thorough examination of the distinct environment at the King Hussein Cancer Centre and the precise circumstances in which the intervention took place. Although our results provide valuable insights, future research should investigate other aspects to further our comprehension of computer-based teaching methodologies in various clinical contexts.
ConclusionThe results showed that computer-based and face-to-face teaching strategies are considered effective strategies for teaching, as both showed a significant increase in the knowledge in each group. In conclusion, our study highlights differences in the effectiveness of computer-based and face-to-face instruction for newly hired oncology nurses in clinically related courses. The results indicate that both instructional methods were effective in increasing knowledge levels among participants. Importantly, the data suggested differences in knowledge retention, with the computer-based instruction group showing a statistically significant advantage over the face-to-face instruction group. While these findings point to variations in instructional outcomes, we refrain from asserting a definitive superiority of one method over the other. Instead, we acknowledge the nuanced nature of educational effectiveness and encourage further exploration of the contextual factors influencing instructional impact in nursing education.
DeclarationThis submission is an original manuscript not been published or submitted for publication in whole or part to any other publishing source.
Ethical considerationApproval for conducting the study was obtained from the Institutional Review Board (IRB) of (King Hussein Cancer Center), ensuring that all ethical considerations were met before the commencement of data collection. Informed consent was obtained from all participating newly hired nurses.
We are grateful to the Science Health Education (SHE) Center and Dana-Farber Cancer Institute for their guidance in editing and review of this manuscript. Special thank you to Editor, Elizabeth Hamlin, for her contribution to the finalization of this manuscript.



