


Academic underachievement is a common presenting symptom and has many different causes. The disorders that describe academic underachievement are based on the child’s function in cognitive, academic, or behavioral domains. The disorders that are associated with academic underachievement are final common pathways that have different etiologies and mechanisms. Multiple disorders are the rule because brain dysfunction in childhood usually affects multiple functions. Consequently, management programs must be individualized, comprehensive and address issues related to the child, school, and family. Treatment plans include parent training, academic accommodations, techniques to maintain self-esteem, and psychopharmacologic approaches. Ongoing monitoring of the management programs is necessary to detect important comorbidities that may emerge, to modify the program to meet the changing academic and social demands that occur as the child ages, and to provide current information. The outcome for children with academic underachievement is most dependent on the underlying disorder. Health providers have multiple roles to play in the prevention, detection, diagnosis and management of children with academic underachievement.
Academic underachievement refers to poor function in the classroom. Although academic underachievement is thought by many to be an educational problem because it occurs in the classroom, physicians have a substantial role to play in the evaluation, diagnosis, management and treatment of children with academic underachievement. Academic underachievement is a common presenting symptom that confronts pediatricians and is one of the most common reasons for consultation of child neurologists, psychiatrists, neurodevelopmentalists, and psychologists. In the United States, 13.4% (NCES, 2010) of children receive special education services. The purpose of this review is to present a clinical approach to academic underachievement.
Academic underachievement is a final common pathway that may result from multiple etiologies. It is a symptom that takes many different forms. It may be confined to a single area of function or it may affect many functions. It may have multiple forms of expression and may be associated with behavioral disturbances. The clinical picture results from the interplay of multiple diagnoses of differing severity, characteristics of the child, the nature of the school, and the abilities of the family. Often, the full picture is not obvious after a single visit. Multiple visits across time may be required to understand the interactions and diagnoses that underlie the academic underachievement.
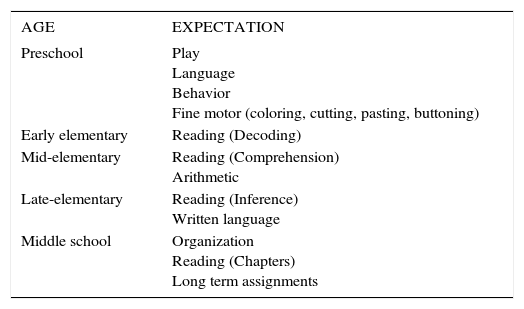
PresentationsAcademic underachievement does not present randomly. Most commonly, the child is brought to attention when he/she cannot meet the expectations of the classroom. Table 1 lists academic expectations that may result in referrals for academic underachievement.
Academic expectations by school placement
| AGE | EXPECTATION |
|---|---|
| Preschool | Play Language Behavior Fine motor (coloring, cutting, pasting, buttoning) |
| Early elementary | Reading (Decoding) |
| Mid-elementary | Reading (Comprehension) Arithmetic |
| Late-elementary | Reading (Inference) Written language |
| Middle school | Organization Reading (Chapters) Long term assignments |
The failure to meet academic expectations may be associated with behavioral disturbance, which may be quite severe. In some children, the behavioral disturbance predominates the picture. Behaviors that are seen commonly include hyperactivity, inattention, sadness, worry, and disruption. It isn’t until the cause of the behavioral disturbance is determined that the academic underachievement is appreciated. For example, a child may be diagnosed as Oppositional-Defiant Disorder until it is recognized that the child has a Mixed Receptive-Expressive Language Disorder and is unable, and not unwilling, to complete her school work.
Behavior disturbance may be noted in the classroom and not the home. Parents of young children often accommodate the child’s deficits and do not put the same demands on them as the classroom. It is important to recognize that children who elope from the classroom are often stating that the current situation is unbearable. Some children even voice suicidal ideation. On the other hand, some children maintain their composure during class and not evidence behavioral disturbances until they are at home-often in conjunction with homework.
Other children come to attention because of an associated dysfunction that causes them to be at risk of academic underachievement. For example, children who are born very prematurely, or have suffered traumatic brain injury, or have epilepsy are all at greater risk of academic underachievement. Many of these children are identified as having school problems before the academic underachievement is fully manifested because of the increased surveillance applied to them.
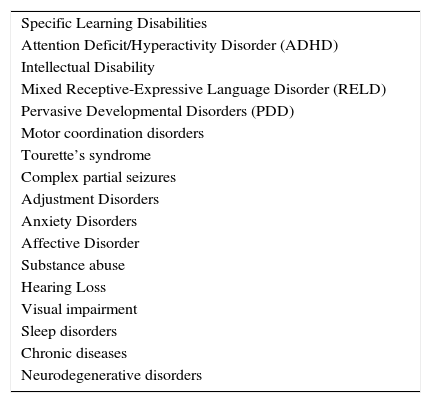
Differential diagnosisThe disorders associated with academic underachievement encompass neurological, behavioral, and emotional disorders and are defined by the functions that they limit. Each of these conditions is associated with many different etiologies. Genetics, trauma, infection (including in utero), toxic exposures (tobacco, alcohol, lead, drugs), and prematurity are but some of the etiologies for the conditions associated with academic underachievement. Because these etiologies cause diffuse brain dysfunction, multiple conditions may be present in the same child. Table 2 lists the differential diagnosis of academic underachievement.
Differential diagnosis of academic underachievement
| Specific Learning Disabilities |
| Attention Deficit/Hyperactivity Disorder (ADHD) |
| Intellectual Disability |
| Mixed Receptive-Expressive Language Disorder (RELD) |
| Pervasive Developmental Disorders (PDD) |
| Motor coordination disorders |
| Tourette’s syndrome |
| Complex partial seizures |
| Adjustment Disorders |
| Anxiety Disorders |
| Affective Disorder |
| Substance abuse |
| Hearing Loss |
| Visual impairment |
| Sleep disorders |
| Chronic diseases |
| Neurodegenerative disorders |
What role should a physician play in care of a child with academic underachievement? If viewed from the limited perspective of school, the answer is minimal. If viewed from the perspective of child health, there are multiple roles that physicians can assume. These roles include prevention, early diagnosis, confirmation of diagnosis, evaluation of etiology, evaluation of associated dysfunctions, treatment, and advocacy for the child.
Prevention of conditions that result in brain injury is a primary role of physicians. Immunizations, nutritional supplementation, protective head gear, auto safety seats, use of seat belts, tobacco and alcohol prevention programs are some of the public health approaches that serve to decrease the conditions that cause academic underachievement. Early diagnosis refers to the pre-academic identification and intervention of conditions that are associated with academic underachievement. Developmental surveillance that focuses on achievement of developmental milestones, particularly language, behavior, and play skills is the initial step in the diagnostic process.
Confirmation of diagnosis is the role that physicians are most frequently asked to perform. Acute and neurodegenerative disorders must be excluded. Often referral for appropriate consultations (psychological, educational, speech and language) is required to establish the diagnosis. Medicine is the only discipline that focuses on determining the etiology of the condition responsible for the academic underachievement. While there is no evaluation guideline for academic underachievement, such guidelines exist for conditions such as Intellectual Disability, Pervasive Developmental Disorder, and Global Developmental Delay.
Physicians have several roles to play in the treatment of children with academic underachievement. First is the appropriate use of medication. Second is advocating for the child. Often, the child with academic underachievement is considered lazy or oppositional. Advocacy by the health provider may help the teacher recognize that the child is unable rather than unwilling. Third is monitoring of the management program. Comprehensive management programs are complex and may need to be adjusted. As the child matures, objectives may need to be altered and the program modified to meet the new requirements.
As noted previously, multiple diagnoses are the rule when evaluating the child with academic underachievement. Failure to identify a significant coexisting condition (e.g., ADHD in a child with specific learning disability) is the most common reason for failed treatment programs. Thus, an important role for physicians is the recognition, diagnosis, and management of associated dysfunctions.
Medical evaluationThe medical evaluation of the child with academic underachievement is wide ranging and should be able to answer the following questions:
- 1.
Is this condition chronic or of new onset?
- 2.
What are the most likely diagnoses?
- 3.
What is the most likely etiology?
- 4.
What confirmatory tests are needed?
- 5.
Is medication management indicated?
A detailed history is the most important part of the medical evaluation, especially defining the nature and course of the underachievement. Has the child failed subjects or repeated a grade? Is the difficulty limited to the classroom or does it pervade the child’s life? Is the difficulty specific to one subject (e.g., reading) or broad. Is the issue related to behavior in the classroom, failure to grasp the material, or difficulty with organization and processes, or a combination? Is the child’s performance variable on a day to day basis? It is important to remember that a clear point of onset suggests an acute disorder.
Capitalize. How long does it take to complete? Does the child dawdle through his homework or have difficulty grasping the concepts? Is the child able to work independently or does he require direct supervision for all of his homework Is all of the work brought home? Is it all submitted when required?
Behavioral history should include measures of inattention and hyperactivity/impulsivity. Mood, anxiety, perseveration/stereotypies and ability to modulate responses (humor and anger) should be evaluated. The review should include performance with peers during extracurricular activities and independent play.
Family history (siblings, parents, grandparents, uncles, aunts, and cousins) of academic difficulties in the early grades, ADHD, anxiety, or affective disorder may provide important information about etiology. Early history should focus on conditions during gestation, labor and delivery that are associated with neural dysfunction. Conditions that may be associated with neural dysfunction, e.g., seizures, infection, or traumatic brain injury or concussion, should be noted. The developmental history is also vital to the assessment. Was there delay in achieving early developmental milestones or unusual behavior as an infant or toddler? Is the child clumsy? Does he have tics? A comprehensive review of systems should provide information about other chronic conditions that may be causing academic dysfunction.
The physical examination should be complete and thorough. It should note growth parameters (especially head circumference), dysmorphisms, skin lesions, and include a complete neurological examination. Soft neurological signs are non -localizing, maturational signs, that are associated with academic underachievement. They are useful in amplifying disorders of tone, symmetry or coordination. Screening of vision and hearing is warranted.
Developmental disorders associated with academic underachievementIntellectual DisabilityIntellectual Disability, previously called Mental Retardation, is the justification for the founding of special education. The most authoritative definition of intellectual disability is that of the American Association on Intellectual and Developmental Disabilities (AAIDD). It defines intellectual disability as a disability characterized by significant limitations both in intellectual functioning and in adaptive behavior, which covers many everyday social and practical skills, and originates before the age of 18. All three principal components of the definition (impaired intellect, adaptive skills, and age) must be present before the diagnosis may be established.
Significant limitation in intellectual functioning is usually measured by a formal, standardized, individually administered test of intelligence. These are typically administered by a psychologist. Significant limitation is felt to be present if the child’s function is more than 2 standard deviations below the mean, and the standard error or measurement is considered. For an IQ test that has a mean of 100 and a standard deviation of 15 points, such as the Wechsler series, an IQ test of 70, or as high as 75, indicates a significant limitation in intellectual function. If one takes the standard error of measurement into account, scores as high as 75 may meet criteria for intellectual disability.
Adaptive behavior deficits are required for the diagnosis of intellectual disability, but are present in many other causes of academic underachievement. Deficits in adaptive behavior are the most controversial aspect of the AAIDD definition because the construct of adaptive behavior is still evolving and there is no universal agreement on how to implement the definition. The current paradigm comprises three skill types: conceptual, social, and practical skills. Conceptual skills focus on language and literacy; money, time, and number concepts; and self-direction. Practical skills include the activities of daily living (personal care), occupational skills, healthcare, travel/transportation, schedules/ routines, safety, use of money. Social skills refer to interpersonal and play skills, self-esteem, gullibility, naïveté (i.e., wariness), social problem solving, and the ability to follow rules/obey laws and to avoid being victimized. Intellectual disability requires significant deficits in one of the three types of adaptative skills.
The final component is age of onset before 18 years. This does not require that the diagnosis be made before 18 years of age, just that there is evidence of intellectual and adaptive behavior deficits before age 18.
There is a range of abilities within the construct of intellectual disability. This is reinforced by epidemiological studies that compare the prevalence of intellectual disability across countries. Severe intellectual disability (IQ<50) is surprisingly stable with a prevalence of about 4 per thousand. By contrast the prevalence of mild intellectual disability ranges from 5-30 per thousand.
There are several reasons for the variation in the prevalence of mild intellectual disability. First, intellectual disability is not a stable construct. Children may grow into or out of the diagnosis. Children who initially are diagnosed as specific learning disabled or language disordered may not maintain their rate of cognitive growth and fall into the range of intellectual disability as teenagers. For these children the initial diagnosis impedes the recognition of the intellectual disability. Other children may be initially diagnosed as intellectually limited but with maturation may evolve into a specific developmental disorder. Second, the diagnosis of mild intellectual disability is difficult to make. In younger children there is a disinclination to make the diagnosis, perhaps related to concerns about the diagnosis becoming a “self fulfilling prophecy”. Older children often mirror the behaviors of their normal intellect peers, thus when viewed on a superficial level, they do not stand out as different. They claim to enjoy the same music and have the same interests and objectives as peers. It isn’t until the reasons why or how are explored that the deficits become apparent. Third, the diagnosis of mild intellectual disability may be obscured by other behavior disorders. Many of the children exhibit externalizing behaviors that are the result of inability but are mistakenly assigned the diagnosis of ADHD or oppositional defiant disorder. Some withdraw and are thought to be depressed. Cognitive function should be considered in all children who presenting with behavioral disturbance.
Specific learning disabilitiesSpecific Learning Disabilities are a group of disorders that manifest as academic underachievement despite having adequate academic instruction and are not due to intellectual disability. Specific Learning Disability is defined as “...a disorder in one or more of the basic psychological processes involved in understanding or in using language, spoken or written, that may manifest itself in an imperfect ability to listen, think, speak, read, write, spell or do mathematical calculations....”United States Code (20 U.S.C. §1401 [30]). Specific learning disabilities may be noted in basic reading (decoding), reading comprehension, mathematic calculation, mathematic reasoning, written expression, listening comprehension and oral expression.
There is no optimal way to diagnose specific learning disability (Shapiro 2007). Operationally, there are three ways used diagnose specific learning disability. The most common means is to document a discrepancy between a child’s academic potential as measured by his IQ and his academic achievement as measured by a standardized academic measure. This method uses a cross-sectional approach and requires measures of both IQ and academic achievement. The discrepancy model assumes that IQ is a good predictor of academic achievement for individual children and that IQ and academic underachievement are independent of each other. A second method to diagnose specific learning disabilities is a longitudinal approach that measures the child’s academic performance at two points at time and determines the progress made during that time. The longitudinal method assumes that three months of progress in first grade is equal to three months of progress in 10th grade. The third method is to provide academic interventions to children who are struggling in the classroom and to identify those children who fail to respond to intervention as learning disabled. This interventional approach assumes that if a child responds to additional instruction or intervention, then the difficulty is not significant enough to become a diagnosis or necessarily need continued services.
Specific learning disabilities describe academic dysfunction and may result from different mechanisms. For example, some children do poorly in basic reading (decoding) because of dyslexia, while others have a mixed receptive expressive language disorders and others have ADHD. It is not uncommon to see multiple specific learning disabilities, e.g., basic reading and written expression or mathematic calculation and written expression.
A complete evaluation of the child’s intellectual, academic, emotional, and behavioral status is needed to establish the diagnosis of specific learning disability. Evaluation of intellect alone is insufficient. The child’s academic capacity also must be assessed. Neuropsychologicalapproaches may provide additional information about the mechanism of the disorder but is not required to establish the diagnosis. Diagnosis and treatment of coexisting disorders (e.g., language disorders or ADHD) are necessary to develop a comprehensive management program.
Children with specific learning disabilities may be maintained in the classroom but will not be successful unless appropriate supports are provided. Some interventions focus on improving the child’s areas of difficulty, e.g., direct instruction for reading disability. Other interventions may affect the learning environment, e.g., special seating. Other accommodations may be used to circumvent the disability, e.g., use of calculators, note-takers, word processors with spell-checkers, or oral testing. Hands-on learning experiences and the use of CDs, DVDs, and videos should be encouraged.
Close attention should be paid to the child’s self esteem. “Burn out” is not uncommon in programs that do not meet the child’s needs. Maintaining extracurricular activities are an important component of the management program to allow the child an outlet to interact with peers in settings not affected by their specific learning disability.
Most children with specific learning disabilities ultimately achieve literacy and numeracy, but may have continuing difficulties in academic related activities as adults. Unsuccessful treatment is associated with poor social and economic outcomes.
Mixed receptive-expressive language disorderMixed Receptive-Expressive Language Disorder (RELD) is one of the specific developmental disorders. It is characterized by weakness in language functions but is distinguished from intellectual disability by relative sparing of non-language skills. Children with RELD may have deficits in adaptive function. Expressive Language Disorders are a group of disorders in language production with relative sparing of language understanding and general cognition. By contrast, speech disorders are difficulties producing speech sounds or problems with voice quality.
RELD is a common disorder in preschool children but relatively under recognized in school -aged children. Young children with RELD come to attention because of too few words. Older children may also have limited vocabulary, but more often they evidence difficulty with word recall, inappropriate use of syntax, not producing sentences of developmentally appropriate length or complexity, or inability to retell stories or express complex thoughts. Most often, adolescents come to attention because of difficulties with higher language functions such as inference, humor, irony, idioms and metaphor (Turner 2008).
The diagnosis of RELD in school-aged children is not simple.Most often the children are evaluated by psychologists who are seeking to differentiate RELD from Intellectual disability or Pervasive Developmental Disorder. The diagnosis of RELD is made when there is a discrepancy between language functions and general cognition. It should be noted that psychological tests are not comprehensive in their evaluation of higher language functions and that RELD may be under-diagnosed if tests of language usage and higher function are not included in the evaluation. If there is a clinical suspicion of RELD not elucidated by psychological evaluation, then additional evaluation by a speech language pathologist with expertise in children is warranted.
RELD is closely linked to other classroom functions (McArthur 2001). Children with RELD may have difficulty with learning to read. Some decode but have difficulty with tasks that extend beyond literal comprehension and require the reader to infer meaning. RELD is associated with disorders in written expression. Sometimes children have difficulty with arithmetical word problems.
Behavioral disturbances may be seen commonly in children with RELD (Shapiro 2008). RELD is a common masquerader of ADHD, because the child does not process the language in the classroom and is thought to be daydreaming. As children approach adolescence, the language demands of social interaction increase dramatically and the child with RELD may be excluded by their peers. Adjustment disorders are common in these children because of their inability to achieve and socialize.
Pervasive developmental disordersPervasive Developmental Disorders (PDD) includes high functioning autism and Aspergers syndrome. These disorders are characterized by 1) a qualitative impairment in reciprocal social interaction and 2) restricted, repetitive, and stereotyped patterns of behavior, interests, and activities. High functioning autism is distinguished from Asperger’s syndrome by a history of clinically significant delays in early language development, social interaction, or imaginative play that are present by age 3 years. The prevalence of PDD has increased and now approximates 1% of children. While there may be an increase in PDD, changing diagnostic criteria, diagnostic overshadowing, and increased incentives to make the diagnosis of PDD are all factors that must be considered before it can be concluded that the incidence of PDD has truly increased.
School-aged children with PDD, RELD, and ADHD show substantial overlap in symptoms. Drawing the diagnostic boundaries is difficult as all may show impaired social interaction and all may have peculiatrities of language usage. Some may use language routines to control situations and be perceived as perseverative rather than anxious. Depending on one’s professional discipline, a child who flaps his arms may be showing synkinesis or stereotypic behavior.
The diagnosis is made on the basis of the clinical picture and confirmed by the use of psychological instruments developed to distinguish children with PDD from typically developing children (e.g., Autsim Diagnostic Interview-Revised (ADI-R), Autism Diagnostic Observation Schedule (ADOS)). Most of the children with PDD are diagnosed in preschool but some children are not diagnosed until late elementary school when reading comprehension requires inferences to be made. The American Academy of Neurology has published a practice guideline to assist in the evaluation of children with PDD (Filipek 2000).
Classroom interventions are similar to those for children with RELD and the use of social scripts or visual cues may prove useful. Adaptive behavior is often deficient and should be addressed within the child’s educational program. Children for PDD may be easy targets for bullies. Behavioral disturbance is common and outbursts may be the result of anxiety or frustration.
Attention deficit/hyperactivity disorderAttention Deficit/Hyperacitivty Disorder (ADHD) is characterized by developmentally inappropriate levels of inattention and/or hyperactivity/ impulsivity that has persisted for more than 6 months and had its onset before age 7. For diagnosis, the child must manifest 6 or more of the 9 characteristics of inattention and/or 6 or more characteristics of hyperactivity/impulsivity contained in the Diagnostic and Statistical Manual -IV-TR and present to a significantly impairing degree. There are 4 subtypes of ADHD--primarily inattentive, primarily hyperactive/ impulsive, combined type, and not otherwise specified, that is used when full criteria are not met. Scandinavian authors maintain the relationship with the older construct, Minimal Brain Dysfunction, and refer to disorders of attention, motor control and perception (DAMP).
The diagnosis of ADHD is made by the child’s behavioral characteristics. Ideally, reports from the school and parents are used to ensure that the impairment is significant. Continuous performance tasks, MRIs, electroencephalograms and psychological tests do not establish or exclude the diagnosis. Behavioral checklists (e.g., Vanderbilt, Conners) are useful as first tier evaluations but should not be used as the only criteria for the diagnosis. The Vanderbilt Assessment Report and Follow-up for Parents and Teachers have been translated into Spanish and are available online.
ADHD has many manifestations and is seen frequently in conjunction with other disorders. The main differential diagnostic point is to determine whether the inattention/hyperactivity is arising from a lack of understanding of the material (as might be seen in specific learning disabilities, intellectual disability, or language disorders) or from a primary disorder of attention (ADHD). Failure to identify comorbid disorders and incorporate them into a comprehensive treatment program will yield suboptimal results. Specific Learning Disabilities are often seen with ADHD. In addition to difficulty with learning basic reading (decoding), children with ADHD will experience difficulty with comprehending and remembering details of chapters during middle school. They often have problems learning multiplication tables and other math facts. Finally, they frequently experience difficulty with written language because of coexisting motor coordination disorders (manifested by neurological soft signs), organizing their thoughts, and language disorders. Children with ADHD have higher rates of motor coordination disorders, cognitive disorders, affective disorders, anxiety disorders and adjustment disorders. ADHD is a cardinal feature of Tourette’s syndrome and is often seen in children with epilepsy.
Children who only have ADHD may have multiple problems with classroom processes but usually do not have difficulty with the content or subject matter. In the classroom they have difficulty with timed assignments/tests, disruptiveness, daydreaming, long-term assignments, and with homework collection, completion, and submission). They may have difficulty with social relationships, due in part to difficulty with modulating responses, anger or humor, poor pragmatic skills, excessive competitiveness, disorganization and disruptiveness.
If ADHD is diagnosed, clinicians should be aware of the possibility of coexisting disorders and should undertake to identify and treat them as well (Floet & Schiener 2010). The primary treatment for ADHD is stimulant medication. Stimulants significantly improve the symptoms of inattention and impulsivity and, thus, improve classroom performance of children with ADHD. Accommodations for testing (e.g., extra time or oral examination), written language and organization are often helpful. ADHD is a life-long disorder. While the hyperactivity/impulsivity may lessen with maturation, inattention, poor organization, and coexisting disorders may continue to affect function through adulthood.
Principles of managementMost children with academic underachievement can be successfully managed with a consortium of the parents, school and physician. Older children should also be part of the management team. While the actual management plan must be individualized, several general principles of management should be noted.
Parent trainingParents manage their children’s care. They serve as the major interface between the child and the rest of the world. In order to be effective, parents must be knowledgeable about their child’s disorders. They must be able to deal with the child at home and with the school personnel. They may make suggestions about aspects of the program, must advocate for their child’s needs with the teacher and school and monitor the overall program. Parents must recognize when things are working well and when additional evaluation is needed. The internet, parent groups, and other materials (books, lectures, DVDs, etc) serve to provide the information to the parent. Often there is a need to put the large body of information into context.
Educational accommodationsEducational accommodations may be general such as small classes, preferential seating, or permitting the child to take a break when they think it is needed. Accommodations may be specific such as reading instruction or social skills building groups. Alternatively, some interventions bypass the area of weakness to limit the disability. For example, the use of books on tape, CDs or DVD to present material to children with specific learning disabilities in reading may avoid their falling behind in social studies. Notifying parents and giving children with ADHD an extra day to turn in their homework avoids much distress. Most educational accommodations are empiric. Speaking with parents about what is being used and what works allows practitioners to build a collection of ideas that may be tried with other students.
Self-EsteemChildren with academic underachievement are at extreme risk of developing poor self-esteem. The main developmental task for school-aged children is to achieve in school. Even children who are not failing suffer from not performing as well as they expect. It is important for all children to have a role to play in their classroom. Gifted teachers ensure that this occurs in the classroom.
Children must think that they are the “best in the world” in some area. Whether they are or not is irrelevant. Extracurricular activities are an important part of the child’s management program.
Many children participate in team sports to demonstrate competence. Those who are not as capable in team functions may do well with individual activities such as swimming, jogging, golf, or tennis. Some children opt for art, music, or drama. Restricting extracurricular activities because of poor academic performance is ill advised and usually results in worsening of classroom function.
MedicationMost academic underachievement does not require medication, but for several conditions medication is the treatment of choice. Medications do not cure the underlying disorders, but control symptoms. Consequently, the time that medication is instituted is not critical. Medication is warranted when there is a mismatch between the demands of the situation and the child’s capacities.
Most medication regimens require a single drug. The use of multiple drugs is usually associated with an inappropriate or incomplete treatment program. Medication is unlikely to be successful if the remainder of the management program is not in place or important coexisting conditions are not identified and addressed.
ConclusionAcademic underachievement is common and has many different causes. The disorders that describe academic underachievement are based on the child’s function in cognitive, academic, or behavioral domains. Multiple disorders are the rule. Management programs must be individualized, comprehensive and address issues related to the child, school, and family. The outcome for children with academic underachievement is dependent on the underlying disorder. Health providers have multiple roles to play in the prevention, detection, diagnosis and management of children with academic underachievement.
Acknowledgement: Supported in part by project T73MC17245, Maternal and Child Health Bureau, Health Resources and Services Administration, United States Department of Health and Human Services.
Special thanks to Sarah Risen, MD for her review of the manuscript and helpful comments.
The author declare no conflicts of interest, in connection to this article.